Some people would do better to read what they are opposing before making irrational emotional posts. MG, did you even read the Great Barring Declaration when it came out, or were you one spreading what the propagandists in the mass media were spreading and vehemently opposing it? Most of those opposing it had never even bothered to read it and followed others blindly in opposing it. If it had been followed as an endorsed official policy it would have saved many, many lives. I’ll post it again and you can let everyone know if you still think it is complete nonsense. FYI - There is a great deal of science supporting the role of T cells and long lasting natural immunity gained by previous exposure to Covid and Corona viruses, especially in children’s immune systems. Governmental bureaucrats don’t always get it right and the mass media has censored far too much information that is later shown to be correct.
The Great Barrington Declaration
The Great Barrington Declaration – As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.
Coming from both the left and right, and around the world, we have devoted our careers to protecting people. Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
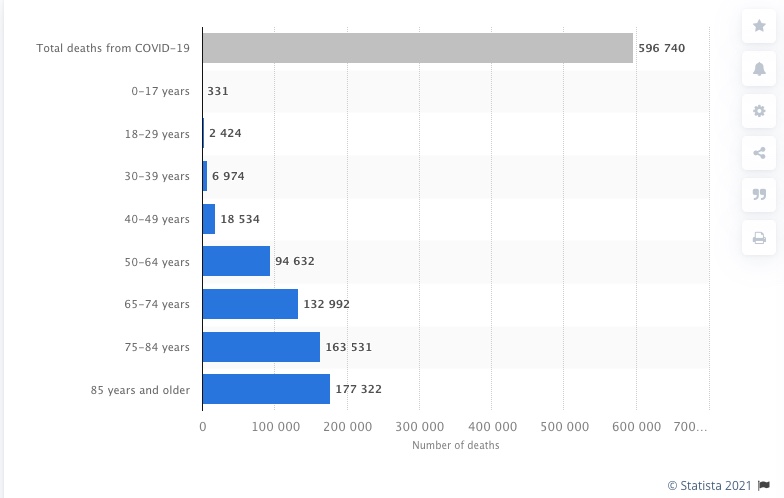
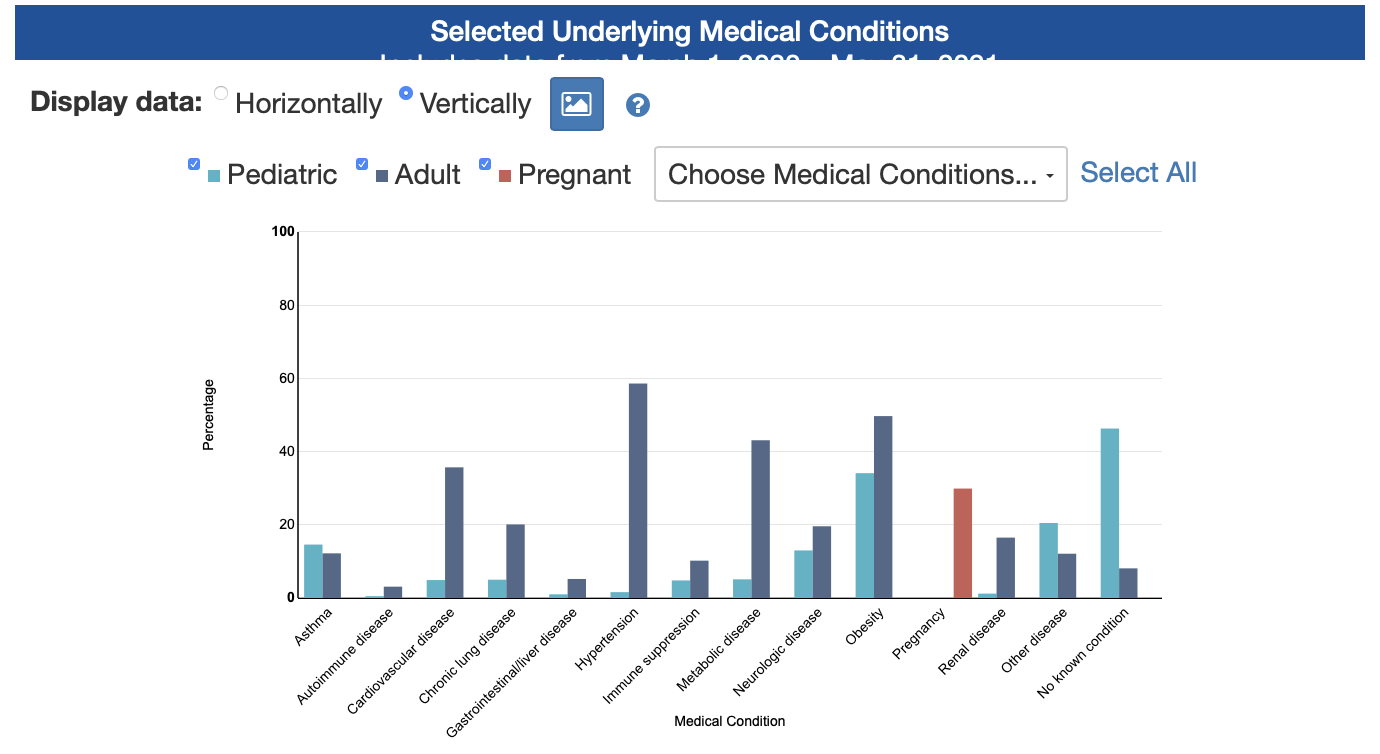
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimize mortality and social harm until we reach herd immunity.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
Adopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent testing of other staff and all visitors. Staff rotation should be minimized. Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.
On October 4, 2020, this declaration was authored and signed in Great Barrington, United States, by:
Dr. Martin Kulldorff , professor of medicine at Harvard University, a biostatistician, and epidemiologist with expertise in detecting and monitoring infectious disease outbreaks and vaccine safety evaluations.
Dr. Sunetra Gupta , professor at Oxford University, an epidemiologist with expertise in immunology, vaccine development, and mathematical modeling of infectious diseases.
Dr. Jay Bhattacharya , professor at Stanford University Medical School, a physician, epidemiologist, health economist, and public health policy expert focusing on infectious diseases and vulnerable populations.
SIGN THE DECLARATION
Co-signers
Medical and Public Health Scientists and Medical Practitioners
Dr. Alexander Walker , principal at World Health Information Science Consultants, former Chair of Epidemiology, Harvard TH Chan School of Public Health, USA
Dr. Andrius Kavaliunas , epidemiologist and assistant professor at Karolinska Institute, Sweden
Dr. Angus Dalgleish , oncologist, infectious disease expert and professor, St. George’s Hospital Medical School, University of London, England
Dr. Anthony J Brookes , professor of genetics, University of Leicester, England
Dr. Annie Janvier , professor of pediatrics and clinical ethics, Université de Montréal and Sainte-Justine University Medical Centre, Canada
Dr. Ariel Munitz , professor of clinical microbiology and immunology, Tel Aviv University, Israel
Dr. Boris Kotchoubey , Institute for Medical Psychology, University of Tübingen, Germany
Dr. Cody Meissner , professor of pediatrics, expert on vaccine development, efficacy, and safety. Tufts University School of Medicine, USA
Dr. David Katz , physician and president, True Health Initiative, and founder of the Yale University Prevention Research Center, USA
Dr. David Livermore , microbiologist, infectious disease epidemiologist and professor, University of East Anglia, England
Dr. Eitan Friedman , professor of medicine, Tel-Aviv University, Israel
Dr. Ellen Townsend , professor of psychology, head of the Self-Harm Research Group, University of Nottingham, England
Dr. Eyal Shahar , physician, epidemiologist and professor (emeritus) of public health, University of Arizona, USA
Dr. Florian Limbourg , physician and hypertension researcher, professor at Hannover Medical School, Germany
Dr. Gabriela Gomes , mathematician studying infectious disease epidemiology, professor, University of Strathclyde, Scotland
Dr. Gerhard Krönke , physician and professor of translational immunology, University of Erlangen-Nuremberg, Germany
Dr. Gesine Weckmann , professor of health education and prevention, Europäische Fachhochschule, Rostock, Germany
Dr. Günter Kampf, associate professor, Institute for Hygiene and Environmental Medicine, Greifswald University, Germany
Dr. Helen Colhoun , professor of medical informatics and epidemiology, and public health physician, University of Edinburgh, Scotland
Dr. Jonas Ludvigsson , pediatrician, epidemiologist and professor at Karolinska Institute and senior physician at Örebro University Hospital, Sweden
Dr. Karol Sikora , physician, oncologist, and professor of medicine at the University of Buckingham, England
Dr. Laura Lazzeroni , professor of psychiatry and behavioral sciences and of biomedical data science, Stanford University Medical School, USA
Dr. Lisa White , professor of modelling and epidemiology, Oxford University, England
Dr. Mario Recker , malaria researcher and associate professor, University of Exeter, England
Dr. Matthew Ratcliffe , professor of philosophy, specializing in philosophy of mental health, University of York, England
Dr. Matthew Strauss , critical care physician and assistant professor of medicine, Queen’s University, Canada
Dr. Michael Jackson , research fellow, School of Biological Sciences, University of Canterbury, New Zealand
Dr. Michael Levitt , biophysicist and professor of structural biology, Stanford University, USA.
Recipient of the 2013 Nobel Prize in Chemistry.
Dr. Mike Hulme , professor of human geography, University of Cambridge, England
Dr. Motti Gerlic , professor of clinical microbiology and immunology, Tel Aviv University, Israel
Dr. Partha P. Majumder , professor and founder of the National Institute of Biomedical Genomics, Kalyani, India
Dr. Paul McKeigue , physician, disease modeler and professor of epidemiology and public health, University of Edinburgh, Scotland
Dr. Rajiv Bhatia , physician, epidemiologist and public policy expert at the Veterans Administration, USA
Dr. Rodney Sturdivant , infectious disease scientist and associate professor of biostatistics, Baylor University, USA
Dr. Salmaan Keshavjee , professor of Global Health and Social Medicine at Harvard Medical School, USA
Dr. Simon Thornley , epidemiologist and biostatistician, University of Auckland, New Zealand
Dr. Simon Wood , biostatistician and professor, University of Edinburgh, Scotland
Dr. Stephen Bremner ,professor of medical statistics, University of Sussex, England
Dr. Sylvia Fogel , autism provider and psychiatrist at Massachusetts General Hospital and instructor at Harvard Medical School, USA
Tom Nicholson , Associate in Research, Duke Center for International Development, Sanford School of Public Policy, Duke University, USA
Dr. Udi Qimron , professor of clinical microbiology and immunology, Tel Aviv University, Israel
Dr. Ulrike Kämmerer , professor and expert in virology, immunology and cell biology, University of Würzburg, Germany
Dr. Uri Gavish , biomedical consultant, Israel
Dr. Yaz Gulnur Muradoglu , professor of finance, director of the Behavioural Finance Working Group, Queen Mary University of London, England