And the beat goes on…“Dutch economist Robin Fransman, the founder of an anti-lockdown group who refused to get vaccinated because coronavirus poses a “minimal risk,” has died of COVID-19. He was 53”
Does long Covid result only from the Covid-19 infection, or can it result from a “leaky vaccine” that has the known side effect of the spiked protein in the vaccine attaching to organs throughout the body, just like the virus itself does? The VAERS system is required by law to report accurately in the National Childhood Vaccine Injury Act of 1986 (see https://www.congress.gov/bill/99th-congress/house-bill/5546). "Sets forth recordkeeping and reporting requirements for vaccine manufacturers. Imposes civil and criminal penalties for destroying, altering, or concealing any such report or record. "
Is the vaccine harmless and without risks? There are over 26,000 deaths reported in VAERS associated with administration of the vaccine. With all other vaccines there is a total of 80! Who in the media is trying to explain this as a misinterpretation of the data?
Okay, only a marketing joke, but there is a larger message behind it. Until recently, the actual package inserts that I’ve personally seen, required by law, were completely blank!
Of special note: “Children COVID-19 mRNA Vaccine BNT162b2 is not recommended for children under 12 years.”
I was only going to post excerpts, but rather than cherry pick the alarming parts, I chose to show the entire insert. You may want to actually read it, as I’m sure few of those administered the jab had this as part of their "informed consent prior to being injected. Now you can finally see the following (if you ask for a copy):
Package leaflet: Information for the recipient
COVID-19 mRNA Vaccine BNT162b2 concentrate for solution for injection tozinameran
This medicinal product has been given authorisation for temporary supply by the UK Department of Health and Social Care and the Medicines & Healthcare products Regulatory Agency. It does not have a marketing authorisation, but this temporary authorisation grants permission for the medicine to be used for active immunisation to prevent COVID-19 disease caused by SARS-CoV-2 virus in individuals aged 12 years of age and over. Reporting of side effects
As with any new medicine in the UK this product will be closely monitored to allow quick identification of new safety information. You can help by reporting any side effects you may get. See the end of section 4 for how to report side effects.
Read all of this leaflet carefully before you receive this vaccine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor, pharmacist or nurse.
- If you get any side effects, talk to your doctor, pharmacist or nurse. This includes any possible side effects not listed in this leaflet. See section 4. What is in this leaflet
What COVID-19 mRNA Vaccine BNT162b2 is and what it is used for
What you need to know before you receive COVID-19 mRNA Vaccine BNT162b2
How COVID-19 mRNA Vaccine BNT162b2 is given
Possible side effects
How to store COVID-19 mRNA Vaccine BNT162b2
Contents of the pack and other information
What COVID-19 mRNA Vaccine BNT162b2 is and what it is used for
COVID-19 mRNA Vaccine BNT162b2 is a vaccine used for active immunisation to prevent COVID- 19 disease caused by SARS-CoV-2 virus.
COVID-19 mRNA Vaccine BNT162b2 is given to adults and adolescents from 12 years.
The vaccine triggers the body’s natural production of antibodies and stimulates immune cells to protect against COVID-19 disease.
- What you need to know before you receive COVID-19 mRNA Vaccine BNT162b2 COVID-19 mRNA Vaccine BNT162b2 should not be given
•
if you are allergic to the active substance or any of the other ingredients of this medicine (listed in section 6). Signs of an allergic reaction may include itchy skin rash, shortness of breath and swelling of the face or tongue. Contact your doctor or healthcare professional immediately or go to the nearest hospital emergency room right away if you have an allergic reaction. It can be life-threatening.
1
PIL BNT162 UK 18_0
Warnings and precautions
Talk to your doctor, pharmacist or nurse before you are given the vaccine if you have:
- ever had a severe allergic reaction or breathing problems after any other vaccine injection or after you were given COVID-19 mRNA Vaccine BNT162b2 in the past.
- you are feeling nervous about the vaccination process or have ever fainted following any needle injection.
- a severe illness with high fever However, a mild fever or upper airway infection, like a cold, are not reasons to delay vaccination.
- a weakened immune system, such as due to HIV infection, or are on a medicine that affects your immune system
- a bleeding problem, bruise easily or use a medicine to inhibit blood clotting There is an increased risk of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the lining outside the heart) after vaccination with COVID-19 mRNA Vaccine BNT162b2 (see section 4). These conditions can develop within just a few days after vaccination and have primarily occurred within 14 days. They have been observed more often after the second vaccination, and more often in younger males. Following vaccination, you should be alert to signs of myocarditis and pericarditis, such as breathlessness, palpitations and chest pain, and seek immediate medical attention should these occur. As with any vaccine, COVID-19 mRNA Vaccine BNT162b2 may not fully protect all those who receive it. No data are currently available in individuals with a weakened immune system or who are taking chronic treatment that suppresses or prevents immune responses. If you are immunocompromised and receive an additional dose of mRNA Vaccine BNT162b2, it may still not provide full immunity to COVID-19 and you should continue to maintain physical precautions to help prevent COVID-19.
Children COVID-19 mRNA Vaccine BNT162b2 is not recommended for children under 12 years. Other medicines and COVID-19 mRNA Vaccine BNT162b2 Tell your doctor or pharmacist if you are using, have recently used or might use any other medicines or have recently received any other vaccine. Pregnancy and breast-feeding If you are pregnant or breast-feeding, think you may be pregnant or are planning to have a baby, ask your doctor or pharmacist for advice before you receive this vaccine. Driving and using machines COVID-19 mRNA Vaccine BNT162b2 has no or negligible influence on the ability to drive and use machines. However, some of the effects mentioned under section 4 ‘Possible side effects’ may temporarily affect the ability to drive or use machines. Do not drive or operate machinery until you are sure that you are not affected. COVID-19 mRNA Vaccine BNT162b2 contains sodium and potassium This vaccine contains potassium, less than 1 mmol (39 mg) per dose, i.e. essentially ‘potassium-free’. This vaccine contains less than 1 mmol sodium (23 mg) per dose, that is to say essentially ‘sodium- free’.
- How COVID-19 mRNA Vaccine BNT162b2 is given
COVID-19 mRNA Vaccine BNT162b2 is given after dilution as an injection of 0.3 mL into a muscle of your upper arm.
2 Ref: PIL BNT162 UK 18_0
You will receive 2 injections, given at least 21 days apart.
If you receive one dose of COVID-19 mRNA Vaccine BNT162b2, you should receive a second dose of the same vaccine at least 21 days later to complete the vaccination series. Protection against COVID-19 disease may not be maximally effective until at least 7 days after the second dose.
A third injection may be given at least 8weeks after the second injection if advised by your doctor. This may also be if your first two doses were with another COVID-19 vaccine.
If you have any further questions on the use of COVID-19 mRNA Vaccine BNT162b2, ask your doctor, pharmacist or nurse.
- Possible side effects
Like all vaccines, COVID-19 mRNA Vaccine BNT162b2 can cause side effects, although not everybody gets them.
Most side effects are mild or moderate and go away within a few days of appearing. If side effects such as pain and/or fever are troublesome, they can be treated by medicines for pain and fever such as paracetamol.
Side effects may occur with following frequencies: Very common: may affect more than 1 in 10 people
• • • • • • •
•
injection site: pain, swelling tiredness
headache
muscle painchills joint pain diarrhoea fever
Common: may affect up to 1 in 10 people
redness at injection site
nausea
vomiting Uncommon: may affect up to 1 in 100 people
enlarged lymph nodes
feeling unwell
arm pain
insomnia
injection site itching
allergic reactions such as rash or itching
feeling weak or lack of energy/sleepy
decreased appetite
excessive sweating
night sweats Rare side effects: may affect up to 1 in 1,000 people
• •
temporary one sided facial drooping
allergic reactions such as hives or swelling of the face3
Ref: PIL BNT162 UK 18_0
Very rare side effects: may affect up to 1 in 10,000 people
• inflammation of the heart muscle (myocarditis) or inflammation of the lining outside the heart(pericarditis) which can result in breathlessness, palpitations or chest pain
Not known (cannot be estimated from the available data)
- severe allergic reaction
- extensive swelling of the vaccinated limb
- swelling of the face (swelling of the face may occur in patients who have had facial dermatological fillers)
- a skin reaction that causes red spots or patches on the skin, that may look like a target or “bulls-eye” with a dark red centre surrounded by paler red rings (erythema multiforme) Some people have reported a sudden feeling of cold with shivering/shaking accompanied by a rise in temperature, possibly with sweating, headache (including migraine-like headaches), nausea, muscle aches and feeling unwell, starting within a day of having the vaccine and usually lasting for a day or two. If your fever is high and lasts longer than three days, or you have other persistent symptoms, this might not be due to side effects of the vaccine and you should seek appropriate medical advice according to your symptoms. Reporting of side effects If you get any side effects, talk to your doctor, pharmacist or nurse. This includes any possible side effects not listed in this leaflet.
If you are concerned about a side-effect it can be reported directly via the Coronavirus Yellow Card reporting site https://coronavirus-yellowcard.mhra.gov.uk/ or search for MHRA Yellow Card in the Google Play or Apple App Store. When completing a report please include the vaccine brand and batch/Lot number if available. Alternatively, side-effects of concern in association with Pfizer BioNTech COVID-19 mRNA vaccine BNT162b2 can be reported to Pfizer Medical Information on 01304 616161 or via www.pfizersafetyreporting.com.
Please do not report the same side-effect(s) to both systems as all reports will be shared between Pfizer and MHRA (in an anonymized form) and dual reporting will create unnecessary duplicates. By reporting side effects, you can help provide more information on the safety of this vaccine.
- How to store COVID-19 mRNA Vaccine BNT162b2
Do not use this medicine after the expiry date which is stated on the box and label after EXP. The expiry date refers to the last day of that month.
Store in freezer at -80°C to -60°C.
Store in the original package in order to protect from light.After thawing, the vaccine should be diluted and administered by a healthcare professional and used within 6 hours. However, in-use stability data have demonstrated that once removed from freezer, the undiluted vaccine can be stored for up to 1 month (31 days) at 2°C to 8°C. Any unused vaccine should be discarded.
- Contents of the pack and other information
What COVID-19 mRNA Vaccine BNT162b2 contains
• The active substance is tozinameran.
After dilution, the vial contains 6 doses, of 0.3 mL with 30 micrograms tozinameraneach.4 Ref: PIL BNT162 UK 18_0
This vaccine contains polyethylene glycol/macrogol (PEG) as part of ALC-0159
• The other ingredients are:
- ALC-0315 = (4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2-hexyldecanoate),
- ALC-0159 = 2[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide,
- 1,2-Distearoyl-sn-glycero-3-phosphocholine,
- cholesterol,
- potassium chloride,
- potassium dihydrogen phosphate,
- sodium chloride,
- disodium hydrogen phosphate dihydrate,
- sucrose
- water for injections What COVID-19 mRNA Vaccine BNT162b2 looks like and contents of the pack The vaccine is a white to off-white solution provided in a multidose vial of 6 doses in a 2 mL clear vial (type I glass), with a rubber stopper and a flip-off plastic cap with aluminium seal. Pack size: 195 vials Manufacturer(s) BioNTech Manufacturing GmbH Kupferbergterrasse 17-19
55116 Mainz, Germany This leaflet was last revised in 12/2021 --------------------------------------------------------------------------------------------- ---------------------------
Oh, never mind, that’s only in the UK. Our package inserts in the US are still blank and not provided to the person receiving the jab!
Yes, the beat goes on.
Dr. Robert W Malone, CO-INVENTOR of the mRNA vaccines (look at the patent, yes there’s a patent), posted on Twitter today that the Pfizer vaccine has been found, a la DATA, to cause more harm than good. Twitter immediately DELETED his account - and he has had to migrate to GETTR. Why can’t we even have a conversation? Oooooops, when the facts are not YOUR side …
And we can all come up with anecdotes - see this one where an Atlanta hospital had GIVEN up on Lou Gossett Jr. He got so angry he discharged himself (could hardly walk out) and took Ivermectin and was better within a couple of days.
https://www.hollywoodlanews.com/lou-gossett-jr-ivermectin-covid/
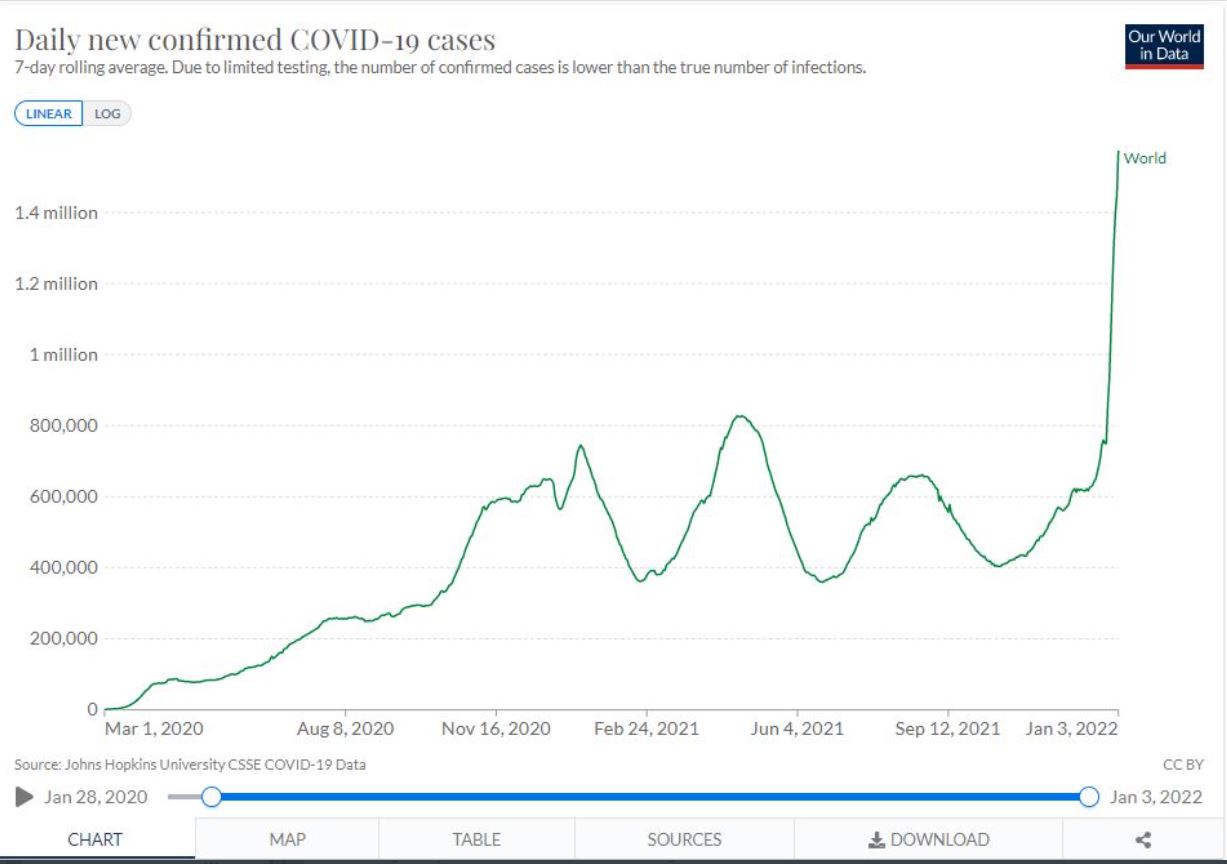
484,377 new cases of COVID today in the U.S. How’s that herd immunity going for you?
Huh? Is there something in the post you tagged concerning new cases or herd immunity?
If so, I don’t see it.
I question and have concern about what Michigan policies have resulted in the worst outcomes in the nation in it’s Covid response this past year!
Tracking Michigan COVID-19 hospitalization data trends
Tracking inpatients, critical care, ventilator data

Michigan hospital data as of Dec. 29, 2021. (WDIV)
Michigan has offered hospitalization data, including inpatients, critical care patients and ventilator use for COVID-19 since April 12, 2020.
Note: As of Aug. 11, MDHHS is reporting both confirmed and suspected COVID-19 cases in hospital data, resulting in an increase in total inpatients. No data was available between Aug. 4 and Aug. 10. ( You can view the MDHHS hospital data page here )
Here’s a look at the state’s hospitalization trends – if you are having trouble viewing the data go here.
![]()
Michigan has a very vulnerable population(aka Detroit area), large sways of the state in rural areas have low vaccine rates and no mask wearing plus perfect virus weather have all combined to create a perfect storm. The Delta outbreak was first driven locally by unvaccinated kids spreading it to their parents but of course now the R0 for Omicron is so high that it is being spread every which way. The next few weeks are going to be the darkest days of the Pandemic for sure but Spring should see the storm over for at least for awhile.
It’s not just about cases and the unvaccinated. Long Covid is of course showing up in the vaccinated as I’ve already pointed out numerous times. As devastating as this virus is, it is taking the course of all Pandemics throughout history and resolving itself on it’s own. Denying there is a small segment of the population that is actually being killed by the vaccines is just nonsense as seen by the VAERS data. Risk of harm vs benefit is something determined on an individual basis in consultation with one’s own physician. Science is increasingly clear on this, even if censored from the public.
The 8% to 12% milder estimate is yet to be determined and possibly much less. The initial 73% prevalence estimate of all new cases by the CDC was revised down to 23% prevalent 1 day ago, and likely to change as time passes. It’s too early to tell just how severe the effects of Omicron will be, but Delta at present is still the dominant variant and more virulent.
Things are rapidly evolving across the country, but it increasingly clear not everyone should blindly receive the EUA vaccines. Not having a package insert with possible side effects in this country is against the law as codified in H.R. 5546 - 99th Congress. Pfizer clearly stated in the UK package insert, “ Children COVID-19 mRNA Vaccine BNT162b2 is not recommended for children under 12 years.” Why is this different in the US? Bureacratic public health policies are creating much more wide-spread harm and confusion than just hospitalizations and deaths.
I disagree with many of the politically biased conclusions and comments of this author, but there is important information to be gleaned as to what is occurring, and the views presented are much the same as appear in MSM.
First they ran short of PPE, then ventilators. Now, the shortage is hospital staff.
By Dan Diamond
‘ROCHESTER, Minn. — Craig Daniels trained for this moment. For nearly two decades, he has worked as a critical care physician at the Mayo Clinic, one of the world’s leading hospitals. His team in the intensive care unit has helped save the lives of hundreds of coronavirus patients.
But amid a seemingly endless pandemic, he admits to some discouraging days.
“There’s this assumption that two years into the pandemic, health care somehow should have hired more people,” Daniels said as patients trickled into Mayo’s snow-dappled campus Wednesday. “But the truth is that we are at the limit. … The people who draw blood. The people who work night shifts. The people who sit in rooms with patients who are delirious. They’re tired. We’re all tired.”
Doctors at this elite institution are confronting the same challenges as their colleagues everywhere: exhaustion, burnout and exasperation at patients who still refuse to mask up and get vaccinated. And that was before the arrival of omicron, the most transmissible variant yet, which is sickening staffers as well as patients and fueling workforce shortages.
Five things about omicron that I want my friends and family to know
As a result, health-care systems nationwide are canceling elective procedures, turning away requests to take emergency medical services patients and grappling with workers calling in sick. Multiple states have deployed the National Guard to help support stressed hospitals, often by simply managing administrative tasks such as helping deliver food or cleaning dirty rooms.
“Frankly, between postponing elective surgeries, delaying surgeries, transferring patients, EMS bypass, and now the National Guard coming in … it’s going to be approaching a breaking point if we don’t turn the tide on these hospitalizations very soon,” said John Palmer, a spokesperson for the Ohio Hospital Association.
The worsening situation has left some doctors fearing that patient care is at risk.
“Our level one trauma hospital — the state’s only one — will be performing ONLY emergency surgical procedures, starting today, to try to preserve our ability to provide high-quality care to acutely ill patients,” Megan Ranney, an emergency physician at Brown University in Rhode Island, wrote in a text message Wednesday.
“Our absences are through the roof. And the patients are so sick — not just with covid but with everything. It’s so, so bad,” Ranney said. “The next few weeks are going to be terrifying for patients and families and providers.”
Omicron appears to cause relatively mild symptoms in many vaccinated people, and while the fast-spreading variant is driving record infections, hospitalizations have lagged behind. But the variant is already exacting a toll on hospitals and their exhausted staff, some of whom are suffering breakthrough infections themselves — and being told they may need to rush back to the front lines.
Worsening staffing shortages prompted the Centers for Disease Control and Prevention (CDC) last week to loosen its guidance for health-care personnel, allowing hospitals to immediately call back infected or exposed workers who have no symptoms, if necessary. The agency had previously recommended that infected health workers isolate for 10 days to reduce the risk of viral spread. Now it says they can return after seven days if they test negative and are asymptomatic — and sooner, if need be, in a “crisis.”
That staff flexibility could be essential given the uncertainties of omicron, said CDC Director Rochelle Walensky, who served as chief of infectious disease at Massachusetts General Hospital for the pandemic’s first year.
“Having been among the health-care workforce … this was something in prior surges that has been really important,” Walensky said in an interview. “While in prior waves, we’d seen ventilators being scarce, supply of dialysis machines, ICU beds, so much of what’s happening with omicron is actually the scarcity of … the health-care workforce itself.”
Hospital associations called the measure necessary and proactive, given the possibility that hospitalizations will spike as omicron moves through the country.
The CDC’s announcement “will help to alleviate the severe workforce shortage crisis facing hospitals across the country,” Nancy Foster, vice president of quality and patient safety policy at the American Hospital Association, said in a statement. “Safely caring for our workforce, patients and communities continues to be our top priority.”
But some health-care workers worry that rushing infected colleagues back to their jobs could pose new risks, such as spreading the virus to uninfected workers and patients.
“Having people come back sick, I don’t agree with that at all,” said Joannie Yeh, a pediatrician who practices outside Philadelphia.
Yeh said she’s particularly worried if providers aren’t given a choice about working alongside infected colleagues. “Would I rather have help from a willing, asymptomatic, covid-positive co-worker who’s going to see covid-positive patients for me, so I can take care of the other patients … than cover everything myself?” Yeh asked. “I don’t think there’s a one-size-fits-all [approach] — I think it has to be a [decision] on the floor level.”
‘There’s no more words’
In Minnesota, local doctors have painted a grim portrait of the worsening pandemic. Cases this month are setting records. More workers are calling in sick. Even Gov. Tim Walz (D) reported a breakthrough infection.
The state’s hospitals issued a full-page plea in local newspapers on Dec. 12, warning residents that “overwhelmed” facilities couldn’t promise patients timely care.
“All the medical-surgical units, beds and spaces are full. Many patients are lined up in the hallways there as well,” said Rahul Koranne, president of the Minnesota Hospital Association. “There’s no more words. I’ve called it a crisis, I’ve called it a catastrophe … calling it a perfect storm is an understatement, but that’s what it is.”
At Mayo, about 100 patients were hospitalized for coronavirus infections or related complications as of Tuesday morning, down from a peak of about 140 hospitalizations earlier in December, but still among the highest levels of the pandemic. Internal Mayo models project that omicron-related hospitalizations will spike in mid-January, although leaders are bracing for the prospect that the new wave will crest sooner.
Daniels, a pulmonologist who helps set the hospital’s coronavirus policies, said he’s particularly worried about omicron’s ability to evade antibodies and infect the vaccinated — including the doctors and nurses whom Mayo desperately needs to deliver care. “Those breakthrough infections almost certainly will include the health-care workforce, which is already strained and already tired and already short-staffed,” he said.
Those concerns are echoed in Rhode Island, where hospital leaders are warning of an “unprecedented crisis” as cases climb amid significant staff shortages. In New York City, health workers say improvements in caring for covid patients matter little if caregivers themselves are spread too thin.
“It’s not March 2020 — we have the testing and treatments and extensive experience treating this disease,” said Craig Spencer, director of global health in emergency medicine at New York-Presbyterian/Columbia University Irving Medical Center. “But if we don’t have the space to treat you, or if we don’t have the providers to give that high quality of care, it might not make a difference if it takes us three times as long to see you in the emergency room.”
Some doctors say they are fighting to fend off feelings of hopelessness.
“It’s difficult trying to remain optimistic,” said Ashley Stantz, a second-year family medicine resident at Mayo. “But I think it’s critical to maintain that optimism because as soon as we lose hope … I don’t know how to recover from that.”
Stantz described a recent covid case involving a middle-aged father with respiratory failure who spent weeks in the ICU, hovering between life and death.
“He told me that I saved his life. And the weight of that was profound,” Stantz said, adding that she has held on to t ‘Still reeling from delta’
All through December, hospital leaders have nervously eyed the nearly vertical increase in omicron infections, worried they will translate into new admissions when there’s little slack in the system.
“Frankly, in many parts of the country, we’re still reeling from delta not yet completing its course,” said Chip Kahn, president and chief executive of the Federation of American Hospitals, which represents about 1,000 for-profit facilities.
While experts acknowledge that hospitals have been hard hit during the pandemic, they say claims about a mass exodus from the profession have likely been overstated, or are part of broader economic trends, such as workers leaving all industries.
“Bottom line is that all health employment is down only 2.7 percent compared to pre-pandemic, and most of that is in nursing homes,” Ani Turner, an economist at the Altarum Institute, wrote in an email, saying there is no data to support an oft-repeated claim that 1 in 5 workers has quit the field.
“Hospital staffing has mostly recovered from the significant drops that happened at the beginning of the pandemic,” said Cynthia Cox, a Kaiser Family Foundation vice president, who co-authored a study that found hospital employment is about 2 percent lower than February 2020 levels and about 4 percent lower than prior projections for December 2021.
“I think the concern right now is, are we heading into a period where everyone comes back from their holiday travels with omicron infection?” Cox added.
Cox and others say they’re looking overseas, to countries such as England where omicron spread earlier, for clues to how the variant disrupted health-care staffing.
But they’re finding scant reassurance there, as scores of U.K. health workers were sidelined with suspected omicron cases earlier this month. Naeema Ginwala-Hasan, an interventional cardiologist who works in London for the National Health Service, said that as her vaccinated colleagues began falling ill, staff were forced to shift more interactions online and additional demands fell on those left behind.
“There’s patient-facing care that still has to happen but it falls on people who haven’t gotten sick yet, unfortunately,” Ginwala-Hasan said. She herself tested positive with a rapid test on Dec. 12, prompting her to isolate from her husband and two children, who she said did not contract the virus.
Federal officials say their new guidance for U.S. health workers is an effort to anticipate and avoid such disruptions, a message echoed by the CDC’s Walensky and other senior Biden administration officials this week.
Brown’s Ranney said she supports loosening restrictions on infected workers, so long as they take proper precautions when they return. But in an interview, she said she’s concerned that protections for health-care workers have been consistently overlooked throughout the pandemic, which she suggested was helping to drive staff shortages.
“It’s become very clear that we may care deeply about taking care of others, but folks don’t actually care all that much about making sure that we’re safe,” Ranney said. “We were told to go to work with bandannas or garbage bags, at the height of the PPE crisis. … And then you’re told that you’re expected to come to work sick, and put yourself and others at risk. It doesn’t compute.”
Daniels, the Mayo Clinic doctor, said he’s disappointed that constant pleas to get vaccinated and take other precautions have failed to win over skeptics — the same people who are disproportionately crowding ICUs. And, as the son of a fireman, he keeps coming back to an analogy from firefighting he tries to understand why health-care workers’ warnings are being shrugged off.
“I tend to be an optimistic person,” Daniels said, but “it amazes me that people want to blame the fire department for the number of fires, rather than the people playing with matches.”
There are a good number of us (probably more than both sides combined) that are able to understand nuance, see merits in arguments from diverging views, and live amicably with others. Partisanship of all kinds is mostly destructive.
3 Likes
Facts and perceptions are important. Science changes as new facts are revealed.
Fauci Now Says Hospitals Are ‘Overcounting’ COVID-19 Cases In Children Because They Automatically Get Tested. Sound Familiar?
By Tim Meads
•Dec 30, 2021
Dr. Anthony Fauci provided some insight regarding the accuracy of metrics used for counting positive COVID-19 cases in children. On Wednesday night, Fauci told MSNBC’s Ayman Mohyeldin that since all children are tested for COVID-19 when they enter a hospital, regardless of the reason they are there, that many children are hospitalized “with COVID” rather than “because of COVID.” Because of that, some COVID-19 cases can be “over counted,” Fauci said.
Keen observers would note that many people skeptical of the official COVID-19 count have argued that exact scenario was happening for quite some time.
As The Washington Examiner reported, Fauci told Moheyldin that childhood COVID-19 cases were rising for a number of reasons, but that doesn’t necessarily mean cause for alarm.
“First of all, quantitatively, you’re having so many more people, including children, who are getting infected. And even though hospitalization among children is much, much lower on a percentage basis than hospitalizations for adults, particularly elderly individuals,” Fauci told the guest host filling in for MSNBC’s Rachel Maddow, “when you have such a large volume of infections among children, even with a low level of rate of infection, you’re going to still see a lot more children who get hospitalized.”
“But the other important thing is that if you look at the children who are hospitalized, many of them are hospitalized with COVID as opposed to because of COVID,” Fauci added. “And what we mean by that — if a child goes in the hospital, they automatically get tested for COVID. And they get counted as a COVID-hospitalized individual. When in fact, they may go in for a broken leg or appendicitis or something like that. So it’s over-counting the number of children who are, quote, ‘hospitalized with COVID,’ as opposed to because of COVID.”
Andy Swan flagged that clip Thursday evening, and sarcastically tweeted, “Fauci regurgitates CONSPIRACY THEORY that ‘hospitalizations’ data is bullshit because most people are in WITH COVID, not FROM COVID.”
“It is absolutely amazing to watch the EXPERTS! class say word-for-word what the banned ‘conspiracy theorists’ were trying to communicate for the past 20 months,” Swan added.
“If you ever wondered if they were lying the whole time, this video puts any good faith claim to rest,” Mike Cernovich opined.
Even in May of this year, researchers at Stanford stated that people were vastly overestimating childhood COVID-19 cases for the exact same reasons that Fauci laid out Wednesday. Fauci — of course — made no mention that over-counting COVID-19 cases was not a novel idea and that others had theorized this was happening before.
A reasonable assumption could be made that if hospitals are doing this for children — and failing to differentiate between patients “with COVID” vs. patients in the hospital “because of COVID” — then it is possible they are doing this for adults as well.
The views expressed in this piece are the author’s own and do not necessarily represent those of The Daily Wire.
The Daily Wire is one of America’s fastest-growing conservative media companies and counter-cultural outlets for news, opinion, and entertainment. Get inside access to The Daily Wire by becoming a member .
I look to multiple sources and try to discern what is actually occurring.
World Council for Health calls for an immediate stop to the Covid-19 Experimental “Vaccines”
Dec 20, 2021
A. CONSENSUS OF WORLD’S FOREMOST EXPERTS
Globally renowned experts, including Dr. Paul Alexander, Dr. Byram Bridle, Dr. Geert Vanden Bossche, Prof. Dolores Cahill, and Drs. Sucharit Bhakdi, Ryan Cole, Richard Fleming, Robert W. Malone, Peter McCullough, Mark Trozzi, Michael Yeadon, Wolfgang Wodarg, and Vladimir Zelenko, among many others, consistently warn the world about the adverse effects resulting from Covid-19 experimental injections; they also warn about their longterm effects, which cannot be known at this time since most clinical trials will be not completed until 2023, and some as late as 2025.
In June 2021, Dr. Tess Lawrie, co-founder of the World Council for Health and member of the Council’s Steering Committee, courageously described the global crisis and called for urgent action: “There is now more than enough evidence on the [UK] Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans. Preparation should be made to scale up humanitarian efforts to assist those harmed by the COVID-19 vaccines and to anticipate and ameliorate medium to longer term effects.”
B. DECLARATION
The World Council for Health declares that it is time to put an end to this humanitarian crisis. Further, the Council also declares that any direct or indirect involvement in the manufacturing, distribution, administration and promotion of these injections violates basic principles of common law, constitutional law and natural justice, as well as the Nuremberg Code, the Helsinki Declaration, and other international treaties.
C. UNCENSORED FACTS
We now know that children are over one hundred times more likely to die from these experimental injections than Covid-19. Injected athletes, globally, are collapsing before our very eyes. In spite of the fact that reporting systems are limited and passive, millions of adverse effects have been recorded, which include death, paralysis, blood clots, strokes, myocarditis, pericarditis, heart attacks, spontaneous miscarriage, chronic fatigue and extreme depression.
See: coronavirus-yellowcard.mhra.gov.uk
See: vaers.hhs.gov
See: ema.europa.eu/en/human-regulatory/researchdevelopment/pharmacovigilance/eudravigilance
See: vigiaccess.org (search covid-19 vaccine)D. VICTIM TESTIMONIES
The World Council for Health acknowledges and respects the experiences and testimony of the victims of this worldwide medical experiment. We also declare and confirm that safe, effective and affordable treatments for Covid-19 exist and should be made available to all who need them.
See: wewanttobeheard.com
See: nomoresilence.world
See: vaxtestimonies.org/enE. NOT SAFE, NOT EFFECTIVE
Recent studies confirm the risks associated with Covid-19 experimental injections. Emerging research establishes that the injections are neither safe nor effective, and, in fact, are toxic. While some of the known ingredients of the injections cause biological harm, it is even more concerning that the unknown and undisclosed ingredients may present an even greater threat to human health.
F. CEASE AND DESIST
The World Council for Health is ethically and lawfully bound to issue this Declaration, demanding that governments and corporations cease and desist from direct or indirect participation in the manufacturing, distribution, administration or promotion of Covid-19 experimental injections.
The Council declares that every living man and woman has a moral and legal duty to take immediate and decisive action to halt this unprecedented medical experiment, which continues to cause unnecessary and immeasurable harm.
G. NOTICE OF LIABILITY
The right of bodily integrity and the right to informed consent are inalienable and universal human rights, which have been trampled by government mandates and corporate imperatives. Thus, the World Council for Health declares that any person or organization directly or indirectly participating in the manufacturing, distribution, administration or promotion of Covid-19 experimental biologics will be held liable for the violation of principles of justice grounded in civil, criminal, constitutional and natural law, as well as international treaties.
.WCH Calls for an Immediate Stop to Covid-19 "Vaccines" | World Council for Health
2 Likes
True Traderich, agree wholeheartedly with what you say, with one proviso. If everybody thought like you, there would be NO issue, people would just move on. There are some people in society who will NOT stop there and move one - they want to PUNISH the unvaccinated, rob them of their education and ability to make a living. Therein lies the rub.
1 Like
It is a little more nuanced than that even. I would suggest that the majority of people who favor mandates don’t want to punish anyone. They want to protect the most vulnerable, themselves, and those who don’t want to be “protected.” That said, there is a minority (vocal at that) on the vaccination side who do one to punish those who don’t comply. And there is a minority on the anti-vax side who want to do the same to the vaccine takers.
1 Like
Well, OK, I’m open-minded and am amenable to considering what you say.
Maybe I’m just an old fogie and am not reading or listening to the right media, but here’s what I’m seeing:
(1) People and even GOVERNMENTS on the vax side saying they want to punish the unvaxxed by taking their jobs and denying them education. Not only that, they are actually DOING it, and
(2) I’m seeing NOBODY on the non-vax side to date saying they want to punish anybody who is vaxxed.
I could be wrong, and will gladly admit same if there is even close to the same amount of hate from the people who do not want the vax in their body - but feel free to inform me. I’d be interested in seeing that - and will definitely apply the SAME pressure/arguments on them that I interpose against the vaccination nazis.
Same as with Science, various sources give a variety of answers. Where is there a balance between Risk of harm and benefit? In other words, where do policies balance (the Risk of harm and benefit to the population) and (the Risk of harm and benefit to the individual)?
Some Real News About Fake News
It’s not just making people believe false things—a new study suggests it’s also making them less likely to consume or accept information.
The rise of fake news in the American popular consciousness is one of the remarkable growth stories in recent years—a dizzying climb to make any Silicon Valley unicorn jealous. Just a few years ago, the phrase was meaningless. Today, according to a new Pew Research Center study, Americans rate it as a larger problem than racism, climate change, or terrorism.
But remarkable though that may seem, it’s not actually what’s most interesting about the study. Pew finds that Americans have deeply divergent views about fake news and different responses to it, which suggest that the emphasis on misinformation might actually run the risk of making people, especially conservatives, less well informed. More than making people believe false things, the rise of fake news is making it harder for people to see the truth.
Pew doesn’t define what it calls “made-up news,” which is a reasonable choice in the context of a poll, but matters a great deal in interpreting it. The term has come to mean different things to different people. It was coined to describe deliberately false articles created by Potemkin news sites and spread on social media. But in a deliberate effort to muddy the waters, President Donald Trump began labeling news coverage that was unfavorable to him “fake news.” (Indeed, Pew finds that Americans blame politicians and their aides, more than the press, activist groups, or foreign actors, for the problem of made-up news.) Now when Trump’s supporters refer to “fake news,” they often seem to mean mainstream news they dislike, whereas when others do so, they mean bogus information spread by fringe actors.
Read: Why bogus news stories are so hard to stop
If Pew’s data are taken to mean that people find this latter category more dangerous than climate change, that is almost certainly an overreaction. As the political scientist Brendan Nyhan wrote in February, summarizing the state of research in the field:
Relatively few people consumed this form of content directly during the 2016 campaign, and even fewer did so before the 2018 election. Fake news consumption is concentrated among a narrow subset of Americans with the most conservative news diets. And, most notably, no credible evidence exists that exposure to fake news changed the outcome of the 2016 election.
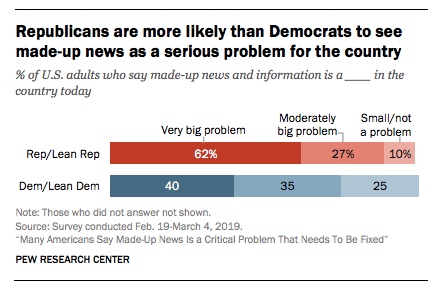
Pew finds a significant gap between Democrats’ and Republicans’ views on the seriousness of the problem with made-up news, though:
This looks a lot like a split over the definition of fake news, rather than the actual problem. Put differently, Republicans may well be responding not to out-and-out fakery, but to bias—real or perceived—in news coverage. It would make sense that conservatives would be primed to accept the idea of widespread bias in the press after a decades-long campaign against the credibility of the mainstream press. Indeed, Republicans are about three times more likely than Democrats (58 percent versus 20 percent) to say that journalists create a lot of fake news, though they still assign more blame to both politicians and activist groups.
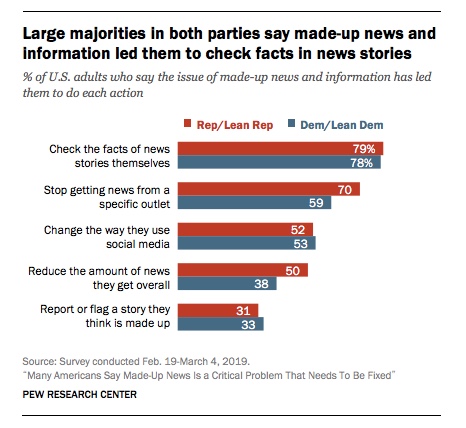
How do people respond when they sense fake news? Here again, the partisan splits are notable:
It’s a positive sign that people are trying to fact-check stories themselves, though it’s an open question whether they’re any good at it. (Respondents thought little of their peers’ ability to find bad information, but believe that they, like the children in Lake Wobegon, are all above average: “Survey respondents also put a good deal more faith in their own ability to recognize potentially inaccurate or misleading information than they do in the broader public’s ability to discern it.”)
Some of the other choices are more troubling. One of the biggest risks often imputed to the current media environment, in which audiences can pick and choose news outlets that agree with them, is that people will become more and more siloed, cutting themselves off from information that they don’t like or that contradicts their prior assumptions.
The Pew study suggests that fake-news panic, rather than driving people to abandon ideological outlets and the fringe, may actually be accelerating the process of polarization: It’s driving consumers to drop some outlets, to simply consume less information overall, and even to cut out social relationships.
If people stop reading a website, because it’s peddling conspiracy theories, that’s good news. If they stop consuming any coverage from mainstream outlets like CNN or The Washington Post , because they believe a story is biased, or because the president has labeled it fake news, that’s less positive. While nearly six in 10 Democrats have dropped an outlet over perceived fake news, a full 70 percent of Republicans have. A much larger portion of Republicans has also reduced their overall consumption of news. The less politically aware are also 20 percent more likely to have reduced their overall consumption of news than the more politically aware—meaning that people who were already acquiring the least information are now acquiring even less.
Fully half of respondents said they had avoided talking with someone, because they thought that person might bring made-up news and information into the conversation. The numbers are roughly equivalent across parties—48 percent of Republicans, 51 percent of Democrats. It’s another example of an action that might seem rational under certain circumstances; no one should feel obliged to listen to an Alex Jones–listening relative’s Sandy Hook trutherism or a neighbor’s Louise Mensch–derived Trump conspiracy theories. But given the relatively small actual prevalence of true fake news, this figure is probably just another sign of people siloing themselves from information that challenges their assumptions.
Nor does Pew’s study offer much reason for optimism that these problems will fade anytime soon. The public’s solutions are fraught with contradictions. More than half of respondents said that journalists bear the most responsibility for fixing the problem (53 percent, versus 20 percent for the public, 12 percent for the government, and 9 percent for tech companies), and yet eight in 10 say limitations on made-up news and information—restrictions on free speech, in other words—are needed. Moreover, almost two-thirds of people said that political divisions are a big challenge to addressing made-up news. Yet the steps that they report taking themselves seem likely to only exacerbate those political divisions.
Deleted after did a fact check…xxxx
For context, I hope anyone reading this last post of mine noticed not only the source, but that it was written pre-Covid-19, and well before the election. Also from the Atlantic, I found this snippet quite interesting. It was actually written the same time as the previous cited article and reprinted recently from the archive. It’s a long informative interview presenting some interesting perspectives, warning of the dangers of AI. I found it very relevant in today’s world of algorithms and “smart” apps. :
Misinformation Is About to Get So Much Worse
A conversation with the former Google CEO Eric Schmidt
By Saahil Desai
Sept 27, 2021
Schmidt: I do think it will be bigger, and the authors collectively disagree on how positive or negative, but we articulate these points in the book. If you look back 20 years ago, people were talking about social networks. No one had any idea that social networks would become so important and would shape the political discourse of elections, how people are treated. It would give a voice to people who are underrepresented but also people we don’t necessarily want to hear from. And we didn’t, at the time, understand the implications of putting everyone on the same network. We need to think now of what happens when artificial intelligence is co-resident with us in the world. It lives with us; it watches us; it helps us, maybe interferes with us occasionally. We don’t really know.Read: Our instructions for AI will never be specific enough
I’ll give you a good example: If you imagine a child born today, you give the child a baby toy or a bear, and that bear is AI-enabled. And every year the child gets a better toy. Every year the bear gets smarter, and in a decade, the child and the bear who are best friends are watching television and the bear says, ’“I don’t really like this television show.” And the kid says, ’“Yeah, I agree with you.” What do we think when humans and these AI systems become best friends? Do we lose our communications and our warmth among humans, or does it get stronger? We don’t know.
(Eric Schmidt: AI Could Worsen Our Misinformation Problem - The Atlantic)
To conserve bits, I’ll leave it there. Read the entire interview if interested.
On another note, Covid related, perhaps you’ve heard some of the recent studies coming out of Denmark about the Omicron surge. Here’s an article from another source that caught my eye this morning. " For example, consuming one or more cups of coffee a day was associated with a 10% decrease in risk of COVID-19 when compared to consuming less than one cup daily. Consuming at least two-thirds of a serving of cooked or raw vegetables daily (excluding potatoes) was also linked with reduced risk." Yes, I am a coffee drinker, among other things. lol
I’m not familiar with the site, so take it for what it’s worth and do your own DD:
COVID NEWS AND COMMENTARY
WHEN ROBOTS ATTACK 
Omicron is spreading like crazy but deaths and hospitalizations are low; the Times shows the new variant seems to have an affinity for the jabbed; the Netherlands goes full booster; and more…
A new preprint Dutch study titled “SARS-CoV-2 Omicron VOC Transmission in Danish Households” found that Omicron is a lot more infectious than Delta. That’s no surprise. But buried in the otherwise obediently pro-vaccine study’s fine print is this little eye-opener:
“Comparing households infected with the Omicron to Delta VOC, we found an 1.17 times higher SAR [secondary attack rate] for un-vaccinated, 2.61 times higher for fully-vaccinated and 3.66 times higher for booster-vaccinated individuals, demonstrating strong evidence of immune evasiveness of the Omicron VOC.”
The higher infectiousness for injected folks is not surprising; we’ve seen that Omicron appears to prefer the jabbed, based on hospitalization numbers and data from areas that track breakthrough cases. But this study shows a significantly higher infection rate for BOOSTED folks, which suggests that the more jabs you get, the more likely you are to catch Omicron, and presumably, any future variant derived from Omicron.
In other words, negative vaccine efficacy may increase with each booster.
A new Canadian preprint study titled “Effectiveness of COVID-19 vaccines against Omicron or Delta infection” similarly found negative efficacy of the jabs against the Omicron variant, especially starting 90 days after the second shot.
That’s when the efficacy goes negative. The study also found protection from Omicron from the second shot dropped to essentially zero after 30 days. Regarding boosters, the study found that while protection increased immediately after receiving the third jab, its efficacy quickly fell to 37% after only seven days following the third shot. Coincidentally, seven days is the length of the only positive study on booster efficacy.
☕️ Coffee & Covid ☙ Tuesday, January 4, 2022 ☙ SHORT SELLING 🦠
Should we be focusing not on “herd immunity,” a misunderstood term, but more on “natural antibody-immunity”? I would describe “natural antibody-immunity” as resulting from a build up of immunity after an exposure to a virus. This type of immunity does not require anything more than a sufficient reservoir of antibodies in a population that lessens severity of any reinfections, or could be preventive against future infections entirely. Natural antibody-immunity better describes the equilibrium that occurs in an endemic of various diseases that we live with year-round, but we never really get rid of either. Endemics are typically treated primarily with therapeutics.
Little chance that COVID will become Endemic into the foreseeable future unless a more effective vaccine is deployed such as the one the U.S. Army is working on.
To discuss further, look at the definition of Endemic:
Note the RO value needs to be essentially one…i.e. one person needs to transmit on average to one other person for it to become Endemic.
COVID-Omicron variety has one of the highest RO values ever discovered. (RO >7) The other variants and future variants will also likely have high RO values especially since it is clear that immunity wanes quickly with this type of virus allowing for individuals to be re-infected over and over again. (4+ infections already in some.) (Note: The high R0 makes it very difficult to control. The R0 of the flu is near 1 which increases to just above that during optimum transmission conditions such as during the Winter. This creates a sort of once a year spike and allows a nice yearly schedule of a vaccine. COVID can strike multiple times a year only slowing down once it has burned through a population till the next variant emerges.)
I think many would like to think that COVID as becoming Endemic as they are so “sick” of it already or are still thinking it will be like the flu. Unfortunately, the coronavirus has other plans and has nothing in common with the flu.
COVID could just as easily be like Small Pox; causing never ending human suffering/death literally for thousands of years unabated without a major therapeutic breakthrough.
Yes, Wikipedia has the classic textbook definition for defining an endemic. Many, including epidemiologists, are more optimistic than that.
Health and Wellness
In a February survey of more than 100 immunologists, infectious-disease researchers and virologists, almost 90% said that SARS-Cov-2, the virus that causes Covid, will become endemic.
That means that there’s a “constant presence and/or usual prevalence of a disease or infectious agent in a population within a geographic area,” according to the Centers for Disease Control. Influenza, for example, is an endemic respiratory illness in the U.S., and there are four other endemic types of coronaviruses that cause the common cold.The Covid pandemic could end next year, experts say — here’s what that looks like, and how the U.S. could get there
Published Thu, Dec 9 20212:32 PM EST
By the end of next year, the Covid pandemic could be over.But that doesn’t mean the coronavirus will disappear. In a blog post on Tuesday, Bill Gates laid out one seemingly likely scenario: “At some point next year, Covid-19 will become an endemic disease in most places.”
If Covid becomes an endemic illness — a disease of relatively low severity that constantly circulates throughout certain parts of the world — the sickness’ pandemic phase could come to a close in 2022, the Microsoft co-founder and billionaire health philanthropist wrote.
…
What living with Covid could look like
Living with Covid will require a shift in mindset, Brewer says: “We have to stop acting like if we do everything right, we’re going to make this virus completely go away.”
Rather, he says, people should try to “minimize the health and economic consequences as much as possible, and get on with our lives.”
In his blog post, Gates agreed. The risk of Covid will hopefully become so low that “you won’t need to factor it into your decision-making as much,” he wrote. “It won’t be primary when deciding whether to work from the office or let your kids go to their soccer game or watch a movie in a theater.”
During the colder parts of the year, some now-familiar prevention measures could remain widespread — like wearing masks in public indoor settings and staying home when you’re sick to prevent spread, Brewer says.
There’s a reason the playbook sounds familiar. “We don’t necessarily have to come up with new interventions [to prevent Covid],” Brewer says. “It’s just that we’ve got to do a better job continuing to do the things we know that work.”
Outbreaks could still emerge in local communities, but the emergence of new antiviral Covid drugs — which aren’t yet approved by the U.S. Food and Drug Administration — could help treat people and prevent the disease from massively spreading again, Gates wrote.
Covid boosters designed to target new variants could also become commonplace, since viruses that continually circulate often mutate into new strains, Gates noted. It’s another familiar idea: Each year’s flu vaccine is already designed for that season’s dominant strains.
I tend to have a more optimistic view of the possibilities then those with a dire outlook.
The only optimism that I see coming from the best/brightest scientists who aren’t political/paid hacks/have hidden agenda’s etc is the likelihood of improved pharmaceutical interventions in 2022. It is unclear how important this will be as those that have chosen not to get vaccinated now probably will not get vaccinated in the future or perhaps even agree to take the new antiviral medications either.
Most are EXTREMELY pessimistic. The biggest reason is the expected onslaught of Long COVID. It appears that Omicron is just as likely to cause Long COVID as other variants but we will see 10X plus the number of infected individuals so the impacts could be devastating. (What happens to those who are already suffering from Long COVID? Does getting re-infected make it worse?) There is no safe group from Long COVID. It is happening to all age groups often regardless of vaccine status or immunity from prior infection.
One of my goals is to get through 2022 without any new brain damage and with my senses of taste/smell in tact. We shall see.
See below. Not much room for optimism from this chart: