194M total infections? certainly a much smaller number than the previous Billions of infections that were being projected a few weeks/months ago.
1 Like
Just for the U.S. i.e. 194 million out 327 million to become infected unless a vaccine becomes available sooner than expected.
Source is NYT - is recent spike in NY deaths possibly due to very restricted access of Dr’s ability to prescribe hydroxychloroquine on a compassionate need basis?
Still have strong doubts about the usefulness of hydroxychloroquine. Note that its usage has been widespread in Italy so certainly no miracle cure. I think controlled studies will show that it has little or no benefit for severe cases but probably it will show benefit in resolving less severe cases quicker which helps with hospital overcrowding. I believe its usage for the H1N1 flu was hyped at one time as well before controlled tests showed 0% benefit. Still, if I come down with the virus, I would hope they give it to me. Not much else, is there?
I think you are correct, it is most useful the earlier it is used in one who has been exposed or infected. For those more severe cases, or those already on a ventilator, a plasma infusion (or gamma globulin) is the best available therapy, which is also available under compassionate use.
Here’s an excerpt from WebMD on an explanation of how it works:
In the UK, Robin May, Professor of Infectious Disease at the University of Birmingham, explained that there is a scientific rationale for the use of hydroxychloroquine in the treatment of COVID-19, based on its mode of action in malaria.
In a statement through the Science Media Centre, he explained that, as chloroquine is a “weak base” and so helps to neutralise acids, it makes the environment “less suitable” for the malaria parasite to live in when it diffuses into red blood cells.
While the mode of action against COVID-19 is not established, Prof May said, he pointed out that many viruses enter host cells via endocytosis, as a result of which they are initially taken up into an intracellular 'compartment that is "typically fairly acidic”.
"Chloroquine would alter the acidity of this compartment, which can interfere with the ability of viruses to escape into the host cell and start replicating.”
He continued: "Another possibility is that chloroquine may alter the ability of the virus to bind to the outside of a host cell in the first place,” adding that the drug "has subtle effects on a wide variety of immune cells…and it may be that one of these effects helps stimulate the body’s ability to fight off COVID-19.”
Crucially, the drug is also “cheap and relatively easy to manufacture” and so could easily be put into clinical trials and, eventually, treatment, May underlined.
A very simple retrospective analysis could be done to see if it has preventative or curative effects. The highest risk group, seniors, are also the group most likely to be taking the drug hydroxychloroquine for Lupus or or Rheumatoid Arthritis. Medicare and Medicaid has an Rx list of those under these programs who have been receiving this drug. The rerospective study would answer the question; “Is the incidence of CCP Coronavirus been reduced from the general population, especially in the Nation’s hot spots?” This study to date has not been undertaken.
Also, part of the rationale for not promoting this drug may be to assure that there was not a shortage. Hydroxychloroquine should be available for those already with an Rx for medical reasons. There is now more availability to use this drug for more than Lupus and Rhematoid Arthritis. For compassionate use an Rx is still needed by a physician. New York is not allowing it’s use for the CCP Coronavirus without going to an Emergency Room first!
Are certain states neglecting seniors by prohibiting appropriate use of Hydroxychloroquine? At least they finally reversed a “bad” decision by their Board of Pharmacy. (Read the entire article, please.) The following is selected excerpts only:
Malaria drug used to treat coronavirus patients at Oregon veterans home
After hearing that hydroxychloroquine could be effective, Dr. Rob Richardson began treating eight of the veterans with it and an antibiotic called azithromycin, also known as Z-Pak.
“I was using it to give them a fighting chance,” Richardson told The Associated Press in a telephone interview.
A doctor at the veterans home in Lebanon used a malaria drug to treat eight patients there for coronavirus, but said a state rule enacted last month would prevent him from treating any more veterans there.
The Oregon Board of Pharmacy had adopted a temporary emergency rule March 25 prohibiting the dispensing of chloroquine and hydroxychloroquine “for presumptive treatment or prevention of COVID-19 infection.”
The board said it took the action to preserve supplies for treatment of malaria, inflammatory conditions, and documented COVID-19 infection in hospitalized patients.
But after pushback against the Oregon Board of Pharmacy’s March 25 rule, the board amended it on Wednesday to allow the drug to be used not only in hospitals for confirmed COVID-19 cases, but also long-term care facilities like the Edward C. Allworth Veterans’ Home.in the second week of March, the first cases of the coronavirusbegan emerging at the veterans home, when two men fell ill with COVID-19. Then more got sick.
Among those treated appears to be William Lapschies, one of the first two confirmed cases. Lapschies celebrated his 104th birthday Wednesday at the veterans home and doctors have declared him fully recovered, said his daughter, Carolee Brown of Lyons.
Malaria drug used to treat coronavirus patients at Oregon veterans home - oregonlive.com
This just came out…no evidence of benefit in severe cases: No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection - ScienceDirect
Are virus base or acid ?
.https://drsircus.com/general/viruses-are-ph-sensitive/ ;
…Now of course you’ll find the negative Nancy postings calling him a quack . Every doctor that went against the established Big Pharm gets labeled that.
The first person that questioned that maybe the body had electrical currents going through it was labeled a quack also. Nobody thinks that of a EKG now.
**A person can test themselves with test PH test strips bought on line, if, you want to see where your body is at.
1 Like
Who Makes Generic Plaquenil?
Generic hydroxychloroquine is made by many different companies, including:
- Mylan Pharmaceuticals
- Sandoz
- Teva Pharmaceuticals
- Watson Laboratories.
A new treatment regimen was used by Dr. Mohammud Alam (an infectious disease specialist) for treating the elderly with CCP Coronavirus. The use of hydroxychloroquine with doxycycline instead of azithromycin is receiving greater attention. Again, read the full article for context, as I extracted only a few details for brevity:
Long Island doctor tries new twist on hydroxychloroquine for elderly COVID-19 patients
“Since we’re talking about the elderly being the most vulnerable, or people with underlying conditions, there is a theoretical benefit of doxycycline over azithromycin because doxycycline is not associated with cardiovascular disease,” said Dr. Sten H. Vermund, the dean of the Yale School of Public Health.
Alam began treating his patients, 45 of whom had tested positive for the coronavirus after they developed a high fever, shortness of breath and cough.
His patients were under long-term acute care and had comorbidities such as hypertension, coronary artery disease, chronic obstructive pulmonary disease or congestive heart failure.
The FDA has warnings that azithromycin “can cause abnormal changes in the electrical activity of the heart that may lead to a potentially fatal irregular heart rhythm.”
“Doxycycline is an anti-inflammatory with properties similar to azithromycin but without the safety concerns and without cardiac toxicity,” he said.
“So I decided why not choose that?” added Alam, a board-certified internist, who shared the results of an observational report consisting of 47 patients he treated.
Again, these patients had tested positive for CCP Coronavirus. It has been shown that patients are best treated with a regimen of hydroxychloroquine in the earlier stages of infections. With elderly patients there can be a very rapid onset of the disease leading to a severe cytokinetic storm. It may be too late in the disease process for hydroxychloroquine to be effective in patients at this stage of the disease. Hospitalization in the ICU for these late stage severe cases may find that convalescent plasma is of greater benefit and may additionally necessitate the use of a ventilator.
Wide-spread mass testing needs to occur, and soon!
A few days ago I started to write a response to several things in the thread, but new information and new models were appearing so rapidly! I was going to start by simply stating that the contagion factor for CCP corona virus is incredibly high. Controlling the rate of how quickly it spreads is useful to model solutions in formulating strategy, policy and treatments. The goal is to minimize the total number of deaths while not exceeding the ability of the healthcare system to treat those who are ill. This must be accomplished without overwhelming the system. Allowing more patients to arrive at the same time than the hospitals can support would destroy healthcare. The public health policies need to concentrate the efforts primarily in the metropolitan areas where the highest population densities exist, and focus on elder care facilities to protect the most vulnerable.
Models are multivariate, focusing on specific areas, and therefore attempt to explain different aspects of the same problem while working towards solutions. This approach results in many models depending on which assumptions predominate. It is now thought that the “COVID-19” corona virus is 3X more contagious than seasonal flu (1.3 RO seasonal flu vs 5.7 RO “COVID-19” - median value from Los Alamos National Lab). It is thought that there are many factors that have slowed the spread of the virus including social distancing, therapeutic measures, and testing to verify presence of the virus, to name but a few. Original unmitigated models showed more than a million deaths in US. With mitigation and other factors, the resulting data predicts fewer deaths from “COVID-19”. The newer IHME model estimates 60K deaths by end of August.
Many models start out by looking at historical data to see if a similar pattern emerges. I’ve looked at how the CDC/FDA had an inaccurate model of the H1N1 virus, but it took years to show how inaccurate this early model was as revealed in their written report three years later.
“The clearest sign of the progress in modeling comes from flu forecasts in the U.S.” Disease modelers gaze into computers to see future of Covid-19 | STAT
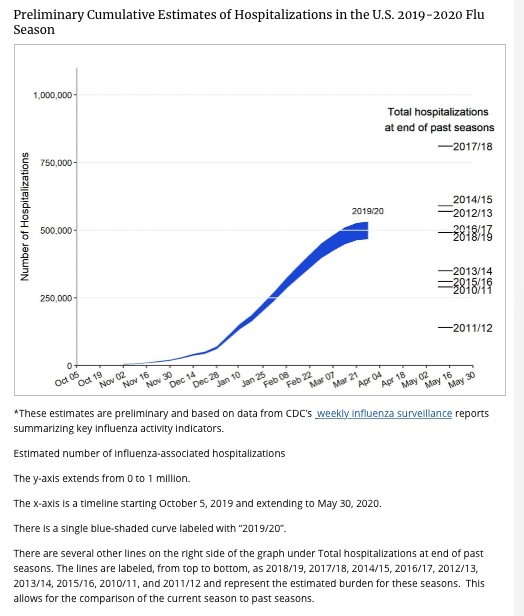
This reminds me of a multi-year graph of hospitalizations from seasonal flu just released by the CDC:
Much of the attention lately has significant misinformation concerning the early use of hydroxychloroquine. That has already been covered ad nauseam, but do look at the previous post and link!
Now to what this post was really going to be about in the first place!
There is a great deal of attention turning to the subject of testing and Abbot’s new testing platform. Abbott’s new m2000 RealTime System received U.S. Food and Drug Administration approval for use in hospitals and molecular laboratories to diagnose the infection. Unfortunately this system is not yet widely being used, or on line, yet. There are 120 certified labs that have this system and test kits, but only 87 are on-line and reporting to the CDC/FDA! According to Dr. Birx, that is being addressed and corrected. So how have approximately 1 million tests or more already been run?
The RT-PCR (reverse transcription-polymerase chain reaction) test is widely used, can be run on a variety of available test kits, and on the older and slower ID Now platforms (Abbott). The ID Now platform is the most common point-of-care test currently available in the U.S., with more than 18,000 units spread across the country. It is widely used to detect influenza, strep throat and other respiratory viruses. Both systems are rapidly ramping up for wide-spread population testing and data collection. Results need to be on line and sent to the CDC to have a comprehensive database!
Between the two platforms, Abbott expects to produce about five million tests per month. It is an RT-PCR type test kit with reagent. The test takes a short segment of RNA and amplifies it to identify the viral pathogen specific to “COVID-19”. Use of the RT-PCR technique identifies the RNA nucleic acids from a nasal swab or nasal wash samples, thereby detecting the active virus, but does not test for the presence of anti-bodies.
You may have already heard there is one Colorado town that has taken a first step into seeing who in their town has the presence of antibodies.
Colorado ski town will test everyone for coronavirus
By Rachael Rettner - Senior Writer
The town will offer coronavirus testing to all 8,000 of its residents, for free.
Town officials will use so-called ELISA tests, which detect antibodies against the new coronavirus in people’s blood. When a person is infected with the new coronavirus, called SARS-CoV-2, their immune system typically develops long-lasting antibodies against the virus within 10 days, ABC news reported. This means antibody tests can reveal what percentage of the population has ever been infected with the virus, even if those tested aren’t currently infected. In contrast, tests used to diagnose the new coronavirus disease, COVID-19, look for SARS-CoV-2’s genes in samples taken from people’s noses and throats, which indicate that a person is actively infected with the virus.
Colorado ski town will test everyone for coronavirus | Live Science
So, with so much new information, do not confuse the RT-PCR Viral test with the antibody tests. The antibody tests are actually quite widely available and being used. These are not yet approved by the FDA for “COVID-19”, although applications have been submitted. There are two methods in use for detecting antibodies. The lateral flow device (LTD) and the enzyme-linked immunosorbent assay (ELISA) have a similar quantitative result. Both are established technologies for detecting DNA in protein specific antibodies. Most of the companies that have IVDs are in the universities or held by private enterprise (corporations).
The FDA Regulates In Vitro Diagnostic Device (IVD) Studies
Updated USFDA guidance issued on March 16, 2020, allows the distribution of many of these types of test kits product for diagnostic use in laboratories or by healthcare workers at the point-of-care.
https://www.fda.gov/media/135659/download
Test kits for the qualitative detection of CCP Coronavirus (“SARS-CoV-2 / COVID-19”) N-Protein IgM / IgG antibodies in human serum, plasma, or whole blood are the gold standard sought for rapid testing. These run on widely available industry standard platforms used mostly for allergen testing in the manufacturing of various products. These antibody tests detect both early marker and late marker, IgM/IgG antibodies in human finger-prick (capillary) or venous whole blood, serum, and plasma samples. This is the basis for the well-known and established ELISA test for detecting components of the immune system. They are investigative at this point for “COVID-19”, but may become widely available relatively soon. Already, there have been 70 submissions for approval to the FDA specifically for “COVID-19” antibody tests that have been developed.
Early investigation shows the highest positive rate of the antibodies against the virus appears 21 - 40 days after the onset, and may have a positive result for years. The IgM is a shorter-lived component that shows up early, and the IgG component remains much longer and is responsible for immunity that may last for years. A titer level, the quantitative concentration of an antibody, is not yet established for “COVID-19” that assures immunity, but is presently being investigated. It is desired that both the RT-PCR and ELISA tests are run together showing if a person has both immunity and no active disease. It is thought that such a ”recovered person” could donate "convalescent” plasma safely and this hypothesis is actively being investigated. Additionally, this dual antigen and anti-body testing would assure that a person could safely return to the work place. Companies could use both these testing methods, RT-PCR and ELISA/LTD, to recommend the appropriate precautions to take in allowing employees to return to work. (The above information is loosely paraphrased from various public sources and some referenced excerpts.)
The nation’s public health policy decisions must first address the issues of containment, treatment and immunity while incrementally allowing an economic recovery to return as quickly and safely as is possible.
Do continue to use safe practices for self and others. Stay well!
EZ
OK, here come three in a row. I’ve put off this post for a few days waiting for someone to post something new. I know the CCP virus is still of great importance to those reading this thread as the coronavirus continues to greatly impact all our lives. I understand there is so much information out there it’s not easy to make a lot of sense out of all of it, let alone focusing in on some of it. Sifting through all the opinions, emotions and media coverage creates quite a controversy. Most of the controversies continue to argue weighing and balancing the different possible policies to prevent the CCP coronavirus from overwhelming the health care system and keeping the population safe. Avoiding continuation of the economic devastation that resulted is finally starting to be addressed in a balanced strategic way. Why has it taken so long? Every wonder why there is a two-week quarantine imposed? Why have we had the 30 day “shelter at home” recommendation imposed nation-wide? Why has there not been wide-spread population testing? Is it reasonable to expect a full implementation of both viral (RT-PCR) testing and antibody (primarily ELISA) testing to allow the economy to recover before resuming most normal activities? I hypothesize the following to answer some of those questions:
Initially, testing and widespread containment measures were imposed with the intent of preventing the healthcare system from collapsing. That goal has largely been achieved. I have some skepticism as to whether this was needed in many of the more rural areas of the country. As best I can tell, several “time targets” are being used to test different hypotheses and set public health policies accordingly. Because “experts” believe there is a maximum and minimum amount of time needed to test whether a potential exposure will result in expression of symptoms that differs from merely the expression of anti-bodies, testing is now moving forward. To be sure, the capability for this testing did not exist, but is rapidly under development.
After an initial exposure the immune system may identify the virus as an “invader” and start producing anti-bodies almost immediately, but not always. The viral RT-PCR test takes as little as 2 days or as many as 10 days to test positive and identifies the presence of the virus. There is some evidence that an additional 3 days past clinical recovery is needed to assure the virus is not still being shed. So how does one test if that is true? What is the quantitative concentration of antibody that attains a protective level? Testing should first be applied to all individuals with symptoms of the flu and Covid-19 in order to distinguish the appropriate diagnosis and treatment.
First, I hope I didn’t over emphasize the need for mass population testing. It probably isn’t necessary, nor is it possible to repeatedly test the entire population as some have suggested. Targeted and intensive testing should be aimed at those areas identified as the most likely vulnerable populations. Results would indicate appropriate measures to prevent and identify potential outbreaks. Small random testing of non-symptomatic populations would map the viral spread. There are major differences between viral RT-PCR testing and the antibody IgM/IgG (ELISA) tests, and what each is actually testing and identifying. The antibody tests actually aren’t that useful for population risk modeling until after the peak hospitalization has started to decline. That “time target” has apparently been reached in many areas. It now makes sense to use and actively perform ELISA testing for the presence of antibodies. Investigators need to determine a titer level that offers protection. How long this protective titer persists also needs to be determined by repeated sampling over extended periods of time.
The risk of an outbreak will be different in different areas of the country. For instance, Idaho on average has a population density of 20 per sq.mi, whereas New Jersey registers 1,200 (List of States By Population Density ). Should the same containment measures be applied in all states for the same length of time? The utility of using these two different tests for mass testing is multi-fold, but may be applied differently regionally. Multivariate analysis will be used to model and consider different variables that may be correlated with each other. It makes sense for both tests to be performed within the workplace for each employee to safely return to work. Both antigen (viral RT-PCR) and anti-body (IgM/IgG, ELISA) tests should first be given to all those currently working and prioritized for healthcare works, first responders, law enforcement, those in public transit work, and other essential jobs.
An anti-body test gives some assurance (in conjunction with a negative RT-PCR test) that a person has “recovered” and can safely return to work. But this broad statement is not entirely true in many instances! What about the individual that had a minor exposure to the virus and successfully creates enough anti-bodies to dispose of the viral invasion quickly? Would this result in a case where the RT-PCR antigen test is negative (no virus) and the ELISA test is positive for the presence of anti-bodies? Is it possible that someone with a very responsive immune system that is repeatedly exposed to low levels of the virus (i.e. some health care workers, average food shopper in metropolitan areas) have increasingly higher levels of anti-bodies due to repeated low-level exposures to the virus? How would we test for this?
The additional information from doing both tests shows how wide-spread the virus has penetrated in the population. However, it does not identify those who have expressed the disease and recovered from those who have only been exposed. Some individuals that have been exposed and produced antibodies have not had a clinical expression of the disease. It may not positively show immunity for those that have had a mild case of the disease. The antibody level in some individuals may not register a sufficient concentration to be protective to future exposures. Multiple small population testing is currently underway and looking to see just how wide-spread the virus exposure is in different parts of the country. We know metropolitan areas are at greater risk of wide-spread contagion than some of the less populated areas.
As already noted, the RT-PCR test takes a significant amount of time, a minimal of several days, to register a positive test, which is one reason for a false negative early on after an exposure. Symptoms of disease generally show up between 2 and 12 days (average is 5-6 days). RT-PCR is the diagnostic test used to confirm the more severe cases - directly tied to hospital reimbursement initially and used to avoid a severe patient overload to some individual hospital systems. That deserves a much longer discussion, perhaps saved for another day. The diagnostic test could have been used more widely if tests were available (they were not) to prescribe medications for those who stayed home with the flu, or those with milder cases of the CCP corona virus. Up until recently, only the severely ill were tested to diagnose if admission to the hospital was necessary, and determine the appropriate treatment regimen to be followed.
So back to the antibody tests … they really don’t measure significant and persistent levels until the immune system has mostly become effective in clearing the virus, roughly 2 weeks to a month and a half after infection. How far are we into the “stay at home” mitigation? Oh, just a little past the one-month mark! It appears mass testing for antibody tests is now starting with a purpose and strategy. Returning people to work safely and providing a reservoir of donors for convalescent plasma to treat other patients can now start in earnest. It appears most geographic areas have nearly reached or passed peak levels of infection and are declining. Is the planned strategy now being employed? These same “donors” would need to be retested periodically for the next year (or longer) to see when a peak titer (quantitative concentration level) has been reached and sustained. There is a problem with incidental low-level exposures that don’t result in expression of the disease; the concentration of anti-bodies circulating in the blood may not be protective against an acute exposure to the virus. Follow-up testing is needed for recovered patients to show if immunity is sustained as indicated by the maximum levels of IgM/IgG antibodies reached and sustained, and that the RT/PCR test is still negative.
Until now, not only were we unprepared to do these type of tests, the data models were only geared to show the worst possible outcome based on retrospective historical models and limited inaccurate “current” information of this pandemic. Current data changed modeling rapidly and “experts” learned more each day. Public health policies were set accordingly, and now need to be adjusted again based on the increased data available nationally and world-wide. Data is still incomplete, however. Some level of mass testing is required not only for determining the lethality of the CCP virus, but the level of penetration and geographic distribution of the coronavirus in the country. Yes, we are ready for strategically sound effective mass population testing of limited size to start. We still don’t know what proportion of the population had milder forms of the disease or those that were exposed and remained asymptomatic. We’ll hear much more on this the next couple of weeks as the ideal “timing periods” have just been reached and passed.
An excerpt from the author’s conclusion of an article that appeared a couple of weeks ago in the NYT states, “ I am deeply concerned that the social, economic and public health consequences of this near total meltdown of normal life – schools and businesses closed, gatherings banned – will be long lasting and calamitous, possibly graver than the direct toll of the virus itself.” The full article titled, Is Our Fight Against Coronavirus Worse Than the Disease? – There may be more targeted ways to beat the Pandemic. By David L Katz, MD
Control of this coronavirus is well underway. Besides testing, many therapeutic treatments are under investigation and engaged in clinical trials; these include Remdesivir, Chlorquine, Hydroxychloroquine, Leronlimab, EIDD-2801 (Ridgeback Biotherapeutics, LP) and Ivermectin to name but a few. (COVID-19 Treatment Update: Remdesivir, Hydroxychloroquine, Leronlimab, Ivermectin, and More ). Coordinated effort to model and find solutions is being led by the COVID-19 High Performance Computing (HPC) Consortium ; members manage a range of computing capabilities that span from small clusters to some of the largest supercomputers in the world. COVID-19 HPC Consortium
This group is Co-chaired by Paul Dabbar (DOE) and Dario Gil (IBM) and includes groups from Industries, US Federal Agencies, Academia and the Department of Energy and National Labs. There is much more coordination going on than the general media reports. Things are progressing well to find solutions. Defeating the CCP coronavirus and returning the nation back to normal life is a priority of effort by all Americans.
Note that an antibody report just came out showing 21% have been infected in NYC with 3 or 4% in the rest of the state. They randomly asked people entering grocery stores for tests. There are likely some problems with the test/methodology but might be the best one done to date. I did a quick review of expert opinion on it and it appears mixed but probably a little on the high side of reality. (The commonly used tests have a high rate of false positives with the error compounded by extrapolating it to the population of the whole city.)
One other thing to note, a follow-up study of those on the princess cruise ship showed I think a majority of those that appeared to be asymptomatic actually had visible lung damage per CT scan that is likely permanent. This completely blows out of the water the notion that most will come down with a “mild” case of the disease as it doesn’t make sense to describe something as “mild” that leaves permanent lung damage!
I think a lot of people are going to be surprised that they have indeed already been exposed to the virus after anti-body tests become wide spread. Since my area is a hotbed of infection, and I had a very extended period of coughing back in January/February, it wouldn’t surprise me if I had an early case of it.
Thanks for posting, Mike.
It is actually not that surprising if there was evidence of pneumonia on the CT images. Why these patients didn’t apparently feel effected by the pneumonia is rather puzzling. Maybe they just weren’t complainers, were too scared to report anything, or just didn’t feel sick? I don’t know that Radiologists would characterize “ground glass” appearance of resolving pnemonia as permanent lung damage. It is a significant finding worthy of reporting and follow-up.
Ground-glass opacity is potentially reversible with appropriate therapy, if the underlying disorder is treated early, because none of the changes in lung structure are permanent.
https://www.ajronline.org/doi/pdf/10.2214/ajr.160.2.8424326
On the NW Coast there was a lot of persistent and unusual respiratory infections in the state of Washington. This was during the height of the flu season during December and January. It was really nasty! Having been in both California and Washington I would note that there was an unusually wet period during February and March. Having spent most of March in Southern California I found this highly unusual. It may be an uncorrelated phenomena that could partly explain and be responsible for a rather low level of severe infections reported on the West Coast. It has been noted in the literature that the virus does not survive well in wet climates (also true of seasonal flu). Additionally, UV (sunlight) will kill the virus on surfaces. As many afternoons turned sunny, not only was the virus deposited on ground and surfaces, it is possible it was totally destroyed as the sunny afternoons dried everything out. Of course, social distancing and masks were also observed by those wanting to protect themselves and others. Regarding the Princess Cruise ship:
For their research, Inui et al. analyzed 112 cases of the coronavirus in patients with an average age of 62 years. The team calculated a severity score for each lung lobe and the entire organ from CT images, comparing asymptomatic (82 cases) and symptomatic (30) patients.
Out of the asymptomatic cases, 54% showed signs of pneumonia; while 80% of CT scans from symptomatic cases showed abnormal findings. Additionally, those without symptoms showed more ground-glass opacity predominance over consolidation. Symptomatic cases more often yielded consolidation.
The authors also noted that asymptomatic images showed milder CT severity scores compared to the others.
Additional investigations will be required, especially to pin-down radiological findings in asymptomatic cases, the group noted.
CT spots COVID-19 lung abnormalities in Diamond Princess cruise ship passengers
There are separate references from Korea/China of CT scans taken at later dates showing what was suggested to be permanent damage. If I come across them again, I will post here.
EDIT: Here is one reference: Explore Bandera County, TX and taste the cowboy spirit
5 questions China should answer to the world…
As the Worlds survival Depends on them.
Consider this as commentary with a few items of news thrown in. Generally, the media does not do a good job, partially because there is just so much information on this virus. There is way more that needs to be done besides the single focus that resulted in an economic shutdown. Much of the crisis facing hospitals is over. There is so much we don’t know about this CCP coronavirus that should not stop the country from returning to a phased in normal. Much of the country still carried on with most essential work during the entire crisis. It is now time to show that the country can “walk and chew gum” at the same time as new problems and challeges show up daily to be met. The economic crisis is looming much larger than the coronavirus now. Both need to be met and overcome.
Admitting patients after a sudden crash is often too late. Recent information suggests Oximetry on an initial evaluation is not only a great idea, but should now be routine. As though there aren’t enough complications associated with this virus, have you heard about this one:
From Barrons:
Mysterious Blood Clots Are COVID-19’s Latest Lethal Surprise
Issam Ahmed and Ivan Couronne
April 27, 2020
…It’s also now clear the COVID-19 illness is associated with an abnormal immune reaction called “cytokine storm” – and some research has indicated this too is linked to higher rates of clotting.
There could also be something about the virus itself that is causing coagulation, which has some precedent in other viral illnesses.
A paper in the journal The Lancet last week showed that the virus can infect the inner cell layer of organs and of blood vessels, called the endothelium. This, in theory, could interfere with the clotting process.
According to Brosnahan, while thinners like Heparin are effective in some patients, they don’t work for all patients because the clots are at times too small.
Much more work is needed in all clinical trials that are underway. I’ve “heard” there are more than 70(?) treatments or clinical trials that have FDA approval under the emergency compassionate use provisions. Some have Federal funding. Let’s hope more than one of these clinical trials brings some good therapeutic, prophylactic, curative or prolonged immunity. There are many in the search to defeat this virus.
That’s why this link is of great interest to me in assuring that the search continues using the best technology available:
This chart was presented by the task force recently:
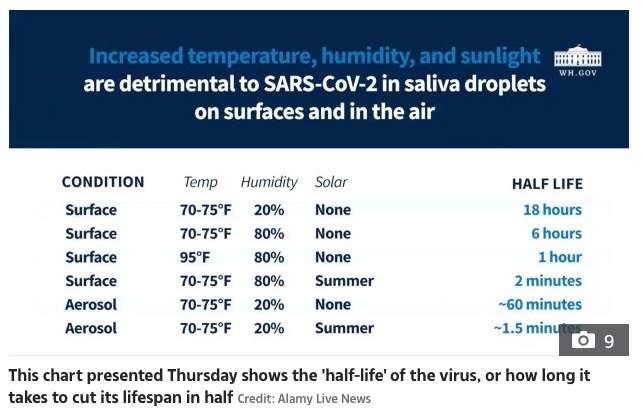
We know there are numerous studies underway by injecting monoclonal antibodies (MABs) or MABs attached to antibodies to target the CCP coronavirus. There is some other surprising research few are aware of, such as injecting a “Disinfectant” into your body.
There is a very short 3 minute video that introduces what this researcher has to say on how Cl02 works generally to cure some diseases, and it’s use as a safe disinfectant that can be ingested if sufficiently diluted:
or go here: Andreas Kalcker - COVER
CHLORINE DIOXIDE FOR CORONAVIRUS: A REVOLUTIONARY, SIMPLE AND EFFECTIVE APPROACH
By A. Kalcker
Posted 21 March, 2020
Every Physician is authorized to use new or unproven preventive, diagnostic and therapeutic procedures according to the HELSINKI WORLD MEDICAL ASSOCIATION STATEMENT – Section No. 37 (This would be the case with chlorine dioxide)
ClO2 aka MMS actually increases oxygen in the bloodstream, Andreas Ludwig Kalcker measured it with venous gasometric tests, It is selective as it works on pH., it activates stem cells in and outside the body, He is working on this research in Switzerland and it will be one of the biggest disclosures in the future of the health field. It does…
Ok, the above link introduces the oral route for treatment of the coronavirus; the somewhat longer 8 ½ minute video link found within the research website below has me convinced that Andreas Ludwig Kalcker is truly an expert that knows exactly what he is talking about. Although the research paper is interesting, it is the video link that looks like the image below you’ll need to look at to see how it relates to the injection of Cl02 to eliminate COVID-19:
https://andreaskalcker.com/en/coronavirus-special-information-for-physicians-and-researchers/
Chlorine dioxide (ClO2) has been used for over 100 years to combat all types of bacteria, viruses and fungi successfully. It acts as a disinfectant, since in its mode of action it turns out to be an oxidant. [1# Biological Efficacy List ] It is very similar to the way our own body acts, for example in phagocytosis, where an oxidation process is used to eliminate all kinds of pathogens.
We are learning more each day on possible solutions to defeat this virus. Early modeling using the dire worst case possible outcomes guided the nation’s early policies. It was what we had to work with at the time. Was it an over reaction? New predictions and policies are being formulated and being implemented. It does not appear the hospital system is in danger of being overwhelmed at the present time by the coronavirus or seasonal flu. Normal healthcare needs to be returned to much of the country. Technology has helped to move things along swiftly and will continue to be applied by numerous groups working collaboratively.
The antibody tests now being developed and applied will target selected groups first, and paired with the viral PCR test, will provide the best information. Medical care to those in need and prevention by detecting early outbreaks is the goal. Both of these kinds of tests have a “sensitivity” deemed unreliable under certain circumstances that is dependent on several factors. In general, the PCR viral test is best at showing a positive result 5-6 days after an exposure. If given earlier it may register as a false negative. The antibody test when given to small random test populations has show there are many asymptomatic individuals that have encountered the virus.This ELISA antibody test is actually most useful about 40 days after a confirmed clinical case of the disease has been resolved. This is because antibodies have generally reached a maximum after this length of time and may confer protection from future encounters with the virus. Much lower anti-body levels may be completely asymptomatic or have resulted from a mild case of the disease. These lower levels may not be protective until a higher concentration of antibody is achieved.
The logical first group to be “dual tested” are those who are directly involved in treating the severe cases. All hospital workers and symptomatic individuals need to be tested, and those at highest risk should have priority with testing until a sufficient number of tests are widely available. Availability of tests are definitely being ramped up to meet the challenge. There is no real need to test every individual.
Those individuals returning to work should be those with lowest risk in the population of having a severe set-back if exposed. Appropriate precautions and testing should be applied within each workplace. Much of the nation is ready to end the shelter-in-place recommendation. Those areas that need to be more cautious will take extra time, but there will always be some risk. Risk vs benefit should always be carefully considered. Let those at lowest risk return to productivity while those at higher risk continue to take necessary precautions. The health system can handle more than just CCP coronavirus cases. Most hospitals are presently underutilized at the expense of not taking care of the normal healthcare needs of patients. Telemedicine is not a substitute for all the health needs of the population.The debate on how best to defeat the threats of this virus are largely geographic. Both healthcare and the economy must return to normal as quickly as possible.
1 Like
Is it time?
Built into the human mind is, a physiological reaction, that, when, we perceive danger we know nothing of, our mind goes into flight or fight response.
This C.C.P. Virius has done just that. … to the world.
Now that we have lived with this virus for months… Maybe it is time we should “assess” if our fears were warranted:
This is insanity! What is the proper response and solution to this virus?
Great post CS! Made me do a little thinking. Who would question great insights from assessments in the general media? Further, why not just remove all “fake news” from such places as youtube and Facebook? Why should anyone subject themselves to viewing such faulty reasoning coming from a couple of frontline doctors actually fighting and dealing with the virus? Are these the only two being censored and removed from public view?
I watched the original interview and have to question whether censorship is increasingly being used to prevent dissemination of truth, or at least chill opposing views. Are Google and Facebook creating a new “book burning” mentality in the digital age by removing non-threatening interviews? People with a brain, even half a brain, can think and reason for themselves without having to rely on “anti stupidy” censorship of the kind apparently being engaged in.
Drs. Dan Erickson and Artin Massihi: Promoting dangerously bogus pseudo-epidemiology about COVID-19
There’s also a pandemic of pseudoscience, misinformation, disinformation, and just plain bad science.
Can we just see who the “author” is?
“DISCLAIMER:: The various written meanderings here are the opinions of Orac and Orac alone, written on his own time. They should never be construed as representing the opinions of any other person or entity"…
Oh my; Much of the this authoratative piece to discredit the video was apparently mis-accredited as seen in the addendum. Admittedly I didn’t absorb the entire discrediting article as I had watched the video before it had been removed from all sources controlled by our favorite news outlets. Maybe I missed something in one or the other.
ADDENDUM: I apparently misattributed Michael Falk’s post. He was quoting someone named Steve Lee, whose original post is here.
Yes, we must not view anything firsthand. I ‘d much rather someone just “report” on what was removed or censored. lol
Steve Lee says:
…6.5% of the people in Bakersfield have or have had COVID-19; i.e., about 58,000 cases, far more than the 700 confirmed cases in the area thus far. He then makes the argument that hospitalization and case fatality rates should be based on these numbers, estimating the COVID-19 case fatality rate to be around 0.02%, arguing that it’s five times less lethal than the 0.1% case fatality rate due to the flu.
Actually, as I recall this has a very minor error. The actual interview I watched said something alarming - the COVID-19 case fatality rate was stated as "0.02” and no percent! I jumped out of my chair to replay it. Dan actually said “0.02” and had mistakenly(?) not included the all important “percent” after 0.02, indeed a rookie mistake! Simple math as a hypothesis … If 100,000 deaths are assumed to occur in the population of 350,000,000, then the resulting death rate is 0.00035 or 0.035%. Of course the entire population will not be exposed. Is 35,000,000 (10%) a more reasonable viral exposure, then the death rate would be 0.35% and, if 15% of population exposed, then 0.23% death rate and, if 20% of the population is exposed, then 0.175% and so on.
Just making a point; In the “original” H1N1 modeling, after 3 months, the initial death rate modeling by CDC was not at all accurate. CDC based modeling on confirmed hospital cases and deaths. When almost 3 years later the statistics were written up to report 274,304 hospitalized, 12,469 deaths and 60.8 million probable cases, it was not reflected in the original data. So, where are we now in CDC modeling? Was the original goal already met? Wasn’t the goal to assure that our hospital system would not collapse and be overrun with more patients than the healthcare system could handle ? Should we reassess if it was worth it and does it continue to make sense? What mistakes were made? Was it based on facts, or purposeful misinformation, and by whom?
Content on this page was developed during the 2009-2010 H1N1 pandemic and has not been updated .
The H1N1 virus that caused that pandemic is now a regular human flu virus and continues to circulate seasonally worldwide.
[CDC H1N1 Flu | Origin of 2009 H1N1 Flu (Swine Flu)]
Note: The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.
Next question I have; Is healthcare still being decimated to keep hospitals from being overrun?
30,000 MAYO CLINIC EMPLOYEES FACING FURLOUGHS OR REDUCED HOURS
“Furloughs will begin in early May and will be spread through the rest of the year, with as many as possible happening through August.
From ABC news - April 24, 2020:
Even nation’s largest health systems laying off health care workers amid COVID pandemic
While private practices and smaller health systems were some of the first to be affected, as time has stretched on, some of the country’s largest health systems have shown that they too are vulnerable.
Yes fake news and misinformation abound! Time magazine reports:
Nearly 70 residents sickened with the coronavirus have died at a Massachusetts home for aging veterans, as state and federal officials try to figure out what went wrong in the deadliest known outbreak at a long-term care facility in the U.S.
The above news isn’t fake … it is a tragedy!
CS, Regarding your 2nd “expose” interview; All I can say is WOW! This doctor might not have everything just right, but he certainly has some interesting views. What if he is right? Well worth watching the entire interview. Has anyone paid attention to NIH, FDA and CDC lately?
NIH partners with 16 drug companies in hopes of accelerating Covid-19 treatments and vaccines:
By LEV FACHER @levfacher - APRIL 17, 2020
W ASHINGTON — The National Institutes of Health on Friday announced it would launch a sweeping public-private partnership between federal researchers and 16 pharmaceutical companies, aimed at coordinating and accelerating the development of Covid-19 treatments and vaccines.
The partnership, to be known as Accelerating Covid-19 Therapeutic Interventions and Vaccines, or ACTIV, is meant to standardize research between the federally funded researchers and a broad array of drug companies, and prioritize research into drugs and vaccines that are having high near-term potential.
Who is aligned with NIH to pick the winners and losers in the fight against the CCD coronavirus? Any conflicts of interest?
FNIH is the Foundation for the NIH, an intermediary that facilitates partnerships between private companies and federal researchers. Who noticed that former NIH Director and Sanofi executive Elias Zerhouni, sits on FNIH’s board. The 16 drug companies involved are: AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Evotec, GlaxoSmithKline, Johnson & Johnson, KSQ Therapeutics, Eli Lilly, Merck, Novartis, Pfizer, Roche, Sanofi, Takeda, and Vir Biotechnology. The information is in plain sight for those who look for it.
OK – Another comment or two about the 2nd video since I’m not yet Brain Dead! Dr. Rashid Buttar’s interview may just have an opposing view, or is it fake news? Can you decide before viewing it? Simply amazing to think a chimeric bioweapon was designed to modify a natural virus dating back to 2014? Pretty deep dive into origins of the origin of this CCP coronavirus! It may at times seem Truth and Disinformation are all the same thing these days! Does whatever you see and hear go into building your knowledge base and view of reality? Who is filtering your reality and making decisions that affect all of us?
People, if you’ve got a brain … can you use it? I don’t need censorship to judge and reason for myself what is factual and what is misinformation. Does what appear as valid information today have a sneaky way of becoming misinformation tomorrow? Usually, an interview is considered opinion; When written up, either to confirm or refute an idea or information, shouldn’t it be factual? Can you tell the validity of something after the original has been censored and removed from sight? Which is opinion and which is fact? Who is to judge? What happens when the average person considers opposing views before it is censored and determines which is truthful? Should a person speak up without fear of reprisal? Does speaking up and having the censorship “punishment” imposed have a chilling effect on all opposing views? Time will tell. It’s up to each of us to make a difference.
One more question I’d like answered. What science is used to determine who is essential and who is non-essential? Apologies for another very long post. My original impulse was to just do a short post from my phone. Perhaps I didn’t need to “sleep on it” and actually review the overwhelming amount of material presented (and now censored) in the public view. Thanks again for posting CS!
Few thoughts…
Actual fatality rate still appears to be around 1%. (For those that try to demonstrate otherwise…think smoke and mirrors, quackery, conspiracy theorists, those with a political agenda, non-scientists.) Bad flu around .1% (Here in Michigan is listed at 9.2% but lot of under counting going on but there are one or two really poorly run hospitals in the Detroit area. Numbers available here: https://coronavirus.1point3acres.com/en ) Attack rate will be around 60 to 80%(flu 10%) which all translates into being about 60 to 80X as bad as the common flu if allowed to run its course. No matter how you slice it, the damage it will do if allowed to run its course will be too high for most of society to accept except those with are just clueless, lack empathy or who are out right psychopaths.
It appears action by many states will indeed cause the virus to run its course. Some are starting to let things reopen despite having more active virus than when they first went into lock down. Crazy?
There will likely be no summer break as it was initially hoped this time around except where lock down measures remain mostly in tact the longest. 2nd (3rd or even 4th) waves are all but certain with the severity of the subsequent waves still in question.
There will be high vacancy rates in nursing homes and prisons in the coming months! Worst job in America going forward…perhaps those working in the meat packing industry?!!
Virus is now the leading cause of death in a number of places. On average of those that die from it, it is shortening their lives by 11 years which is considerable of living lost by almost any standard.
A high percentage of all who get the virus whether one comes down with symptoms or not may suffer lifetime long heath efforts the extent of which remains to be seen. My guess, Americans who are already a pretty sickly lot to begin with as a group will become even more feeble/ill after all is said and done in 18 to 24 months.
Finally, antivirals etc. continue to disappoint/under perform initial expectations. The most “promising” is Remdesivir but based on all the published results thus far and on unbiased expert opinion of those results, it will likely have little or not noticeable impact on the course of the virus. (Think of it in terms of being like AZT for the HIV, helped a little but took another ten years before drugs emerged that really worked.) Having doubts that any treatment will emerge in a meaningful way before the virus runs its course.
P.S. Wear a mask when in any enclosed public space…please?!
1 Like