Heard "Barrington Declaration" mentioned on Sprott’s Weekly Wrap-Up.
Thought it worth posting as the debate continues to weigh all factors that affect daily living with Covid-19 (bolding added for emphasis).
Basically the science by leading scientists, epidemiologists and policy makers remain unsettled.
Thousands of scientists urge end to ‘devastating’ lockdowns
Document cites impact on public health, calls for ‘focused protection’
About 15,000 scientists and doctors worldwide have signed a newly created document urging an end to pandemic lockdowns, arguing that the policies aimed at curtailing the novel coronavirus have produced “devastating” effects on public health.
The Great Barrington Declaration, which was released Tuesday and continues to gather signatures, was spearheaded by doctors from Harvard, Stanford and Oxford University.
“As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection,” said the declaration.
The document argued for allowing most people to “live their lives normally to build up immunity through natural infection,” while improving safeguards for the elderly and others at greater risk of death from COVID-19.
“Coming from both the left and right, and around the world, we have devoted our careers to protecting people,” said the declaration. “Current lockdown policies are producing devastating effects on short and long-term public health.”
They include “lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health—leading to greater excess mortality in years to come.” >
The three lead signatories, who authored the declaration in Great Barrington, Massachusetts, are Harvard professor of medicine Dr. Martin Kulldorf; Oxford epidemiologist Dr. Sunetra Gupta, and Stanford Medical School professor Dr. Jay Bhattacharya.
As of Thursday afternoon, the document had been signed by nearly 5,000 medical and public-health scientists; nearly 10,000 medical practitioners, and more than 128,000 “members of the general public,” according to a tally on the website.
The signers disagreed with those in favor of maintaining restrictions until a vaccine is developed .
“Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed,” the document said.
British Prime Minister Boris Johnson’s government rejected Wednesday the no-lockdowns proposal, with a spokesperson saying it was based on an “unproven assumption,” according to the [U.K.] Independent.
“We have considered the full range of scientific opinion throughout the course of this pandemic and we will continue to do so,” said the Johnson spokesperson.
“But what I would also say is that it is not possible to rely on an unproven assumption that it is possible for people who are at lower risk, should they contract the virus, to avoid subsequently transmitting it to those who are at a higher risk and would face a higher risks of ending up in hospital, or worse in an intensive care unit,” he said.
U.S. shutdown policies vary from state to state, as well as city to city, with California and Hawaii under some of the toughest restrictions and South Dakota, Idaho and Utah with some of the lightest, according to a WalletHub analysis updated Monday.
California Gov. Gavin Newsom drew double-takes last week when his office tweeted a reminder to those going out to dinner to “keep your mask on in between bites.”
It maybe 4 years before things return to “normal” although numerous recent changes in our lives will remain. (For instance, I don’t expect I will ever have to go back working in an office environment.)
On the bright side, this should benefit the price of gold. Also, after it is over; expect a period similar to the roaring 20’s which was caused by the aftermath of the 1918 pandemic. Better, as no reason to think prohibition will come back!
Cause or effect? It appears that states having difficulty opening up are experiencing the highest death rates from China’s Covid caused pandemic.
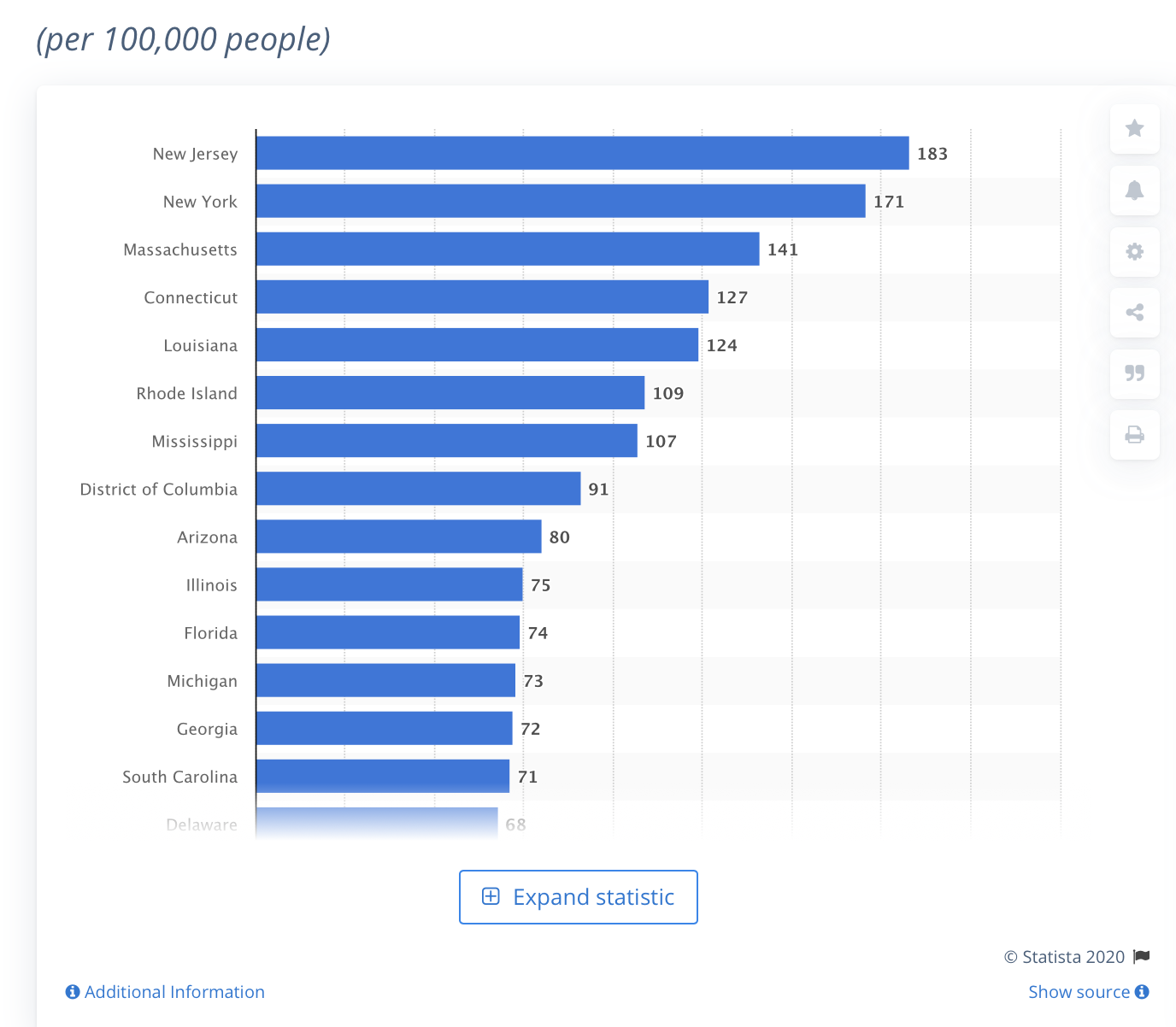
As of October 19, 2020, there have been almost 220 thousand deaths related to COVID-19 in the United States. The death rate from COVID-19 in the state of New York is 171 per 100,000 people. New York is one of the states with the highest number of COVID-19 cases.
Death rates from coronavirus (COVID-19) in the United States as of October 19, 2020, by state
The big news today is a vaccine candidate has been preliminarily shown to be more than 90% effective after taking the 2nd dose. This probably spells the beginning of the end of the pandemic. However, the current new COVID case trajectory in the U.S. is so steep that I’m not sure that there will be that many people who haven’t been infected by the time the vaccine is generally available to the masses sometime later next year. Also, does it actually work for old people/immune compromised individuals? That kind of data is not available.
Some interesting things going on that I had not heard about concerning susceptibility of individuals with certain pathobionts. "The reason for the striking differences in clinical outcomes of SARS-CoV-2 infected patients is still poorly understood. While most recover, a subset of people become critically ill and succumb to the disease." If you don’t know what a Pathobiont is don’t feel bad. I had to look it up. This short excerpt from a much longer article from NIH sums it up pretty well. The article that follows is the one of interest I was not aware of:
Pathobionts of the Gastrointestinal Microbiota and Inflammatory Disease
Abstract
Our immune system is charged with the vital mission of identifying invading pathogens and mounting proper inflammatory responses. During the process of clearing infections, the immune system often causes considerable tissue damage. Conversely, if the target of immunity is a member of the resident microbiota, uncontrolled inflammation may lead to host pathology in the absence of infectious agents. Recent evidence suggests that several inflammatory disorders may be caused by specific bacterial species found in most healthy hosts. Although the mechanisms that mediate pathology remain largely unclear, it appears that genetic defects and/or environmental factors may predispose mammals to immune-mediated diseases triggered by potentially pathogenic symbionts of the microbiota. We have termed this class of microbes `pathobionts’, to distinguish them from acquired infectious agents. Herein, we explore burgeoning hypotheses that the combination of an immunocompromised state with colonization by pathobionts together comprise a risk factor for certain inflammatory disorders and gastrointestinal cancer.
Introduction
Microbes dominate as the most abundant life form on Earth, occupying almost every terrestrial, aquatic, and biological ecosystem on our planet. Humans are no exception. Throughout our lives, we continuously encounter microorganisms that range from those essential for health to those causing disease [1]. The human body is permanently colonized by microbial organisms on virtually all environmentally exposed surfaces. The vast majority of these microbes are harbored in the gastrointestinal (GI) tract where commensal bacteria can outnumber host cells by 10-fold (thus, we are all 90% bacteria on a cellular level). Many vital host functions are provided by the microbiota, including the synthesis of vitamins, digestion of complex polysaccharides, maintenance of the intestinal epithelial barrier, and resistance to pathogen colonization [2]. Millions of years of co-evolution have interdependently linked the health of mammals to their microbiotas [3]. The Human Microbiome Project is currently underway to sequence the microbiota of various populations of people, with a goal of identifying microbial species implicated in health and disease [4]. What is already clear is that microbes have flourished inside us since time immemorial, and have diverged to take on many functional roles that are now being uncovered at the genetic and mechanistic levels. Several descriptions of an intimate link between the microbiota and the immune system have recently emerged [5–8]. However, not all host-microbiota interactions promote health, and particular species of resident bacteria appear to activate the immune system resulting in inflammatory diseases. Thus, our association with the microbial world is precarious.
It is now appreciated that some symbiotic microorganisms in the GI tract induce pathology under certain conditions, usually involving environmental and/or genetic alterations. The term `pathobionts’ has been suggested to describe resident microbes with pathogenic potential [9]. Organisms proposed as pathobionts are associated with chronic inflammatory conditions, unlike opportunistic pathogens which often cause acute infections and are typically acquired from the environment or other parts of the body. In addition, pathobionts are innocuous to the host under normal conditions, distinct from traditional pathogens which may cause disease even in healthy hosts. In this review, we highlight experimental evidence mostly from animal models that support the classification of specific microbes as pathobionts (see Table 1). Furthermore, we explore the role of bacterial pathobionts on intestinal health and their resulting impact on inflammatory bowel disease (IBD) and gastrointestinal cancers.
from articles at NCBI.NLM.NIH (PMC3426444)
Now that a pathobiont has been explained here, the following article should be of great interest to those in the medical community to identify those most vulnerable. It is not just age related.
THE INTESTINAL AND ORAL MICROBIOMES ARE ROBUST PREDICTORS OF COVID-19 SEVERITY THE MAIN PREDICTOR OF COVID-19-RELATED FATALITY
The reason for the striking differences in clinical outcomes of SARS-CoV-2 infected patients is still poorly understood. While most recover, a subset of people become critically ill and succumb to the disease. Thus, identification of biomarkers that can predict the clinical outcomes of COVID-19 disease is key to help prioritize patients needing urgent treatment. Given that an unbalanced gut microbiome is a reflection of poor health, we aim to identify indicator species that could predict COVID-19 disease clinical outcomes. Here, for the first time and with the largest COVID-19 patient cohort reported for microbiome studies, we demonstrated that the intestinal and oral microbiome make-up predicts respectively with 92% and 84% accuracy (Area Under the Curve or AUC) severe COVID-19 respiratory symptoms that lead to death. The accuracy of the microbiome prediction of COVID-19 severity was found to be far superior to that from training similar models using information from comorbidities often adopted to triage patients in the clinic (77% AUC). Additionally, by combining symptoms, comorbidities, and the intestinal microbiota the model reached the highest AUC at 96%. Remarkably the model training on the stool microbiome found enrichment of Enterococcus faecalis , a known pathobiont, as the top predictor of COVID-19 disease severity.Enterococcus faecalis is already easily cultivable in clinical laboratories, as such we urge the medical community to include this bacterium as a robust predictor of COVID-19 severity when assessing risk stratification of patients in the clinic.
As a side note, I started a batch of homemade yogurt this morning with some “good” probiotic to help my intestinal microbiome stay healthy. I’ve enjoyed this as a hobby for quite some time now. Anyone else into making homemade yogurt? I also take all “good sense” appropriate precautions in preventing myself and others from spreading this terrible disease.
It is currently estimated that up to 25% Americans have already gotten the virus which has resulted in 400,000 deaths. Taking into account that the most at risk have either died or will be getting the vaccine soon, or otherwise being more cautious, one could estimate another 600,000 deaths are possible at the high end before this is over. (Actually, it won’t be over in our life times but will become more of a nuisance like a cold/flu and continue to cause travel headaches around the world till well into 2022. )
Current projections are that the average healthy American who isn’t an essential/health work will not have access to the vaccine till September! (Projections have been pushed back recently since the rollout of the vaccines have been way slower than expected and government stockpiles of the vaccines turned out to be imaginary coupled with failing to order the proper amount of vaccine from the manufactures.)
One would think we would see gold prices improve further 2021 with all the pending government spending/currency dilution but bitcoin etc might ruin it. Who knows?
COVID-19 vaccine rollouts are finally upon us. They hope that herd immunity—protection from an infectious disease that occurs once a sufficient proportion of the population has been vaccinated or infected—is on the horizon. But even though the first vaccines to receive emergency use authorization from the U.S. Food and Drug Administration are exceptionally effective at preventing COVID-19, datacannotyet tell us if they hinder transmission of SARS-CoV-2, the virus that causes the disease…
Influenza may provide the best blueprint of what to expect going forward. The most common flu vaccine—the inactivated virus—is not “truly sterilizing because it doesn’t generate local immune response in the respiratory tract,” Crowcroft says. This fact, coupled with low immunization rates (often shy of 50 percent among adults) and the influenza virus’s ability to infect and move between multiple species, enables it to constantly change in ways that make it hard for our immune system to recognize. Still, depending on the year, flu vaccines have been shown to reduce hospitalizations among older adults by an estimated 40 percent and intensive care admissions of all adults by as much as 82 percent.
Research on seasonalcoronaviruses suggests that SARS-CoV-2 could similarly evolve to evade our immune systems and vaccination efforts, though probably at a slower pace. And data remain mixed on the relationship between symptoms, viral load and infectiousness. But ample precedent points to vaccines driving successful containment of infectious diseases even when they do not provide perfectly sterilizing immunity. “Measles, diphtheria, pertussis, polio, hepatitis B—these are all epidemic-prone diseases,” Crowcroft says. “They show that we don’t need 100 percent effectiveness at reducing transmission, or 100 percent coverage or 100 percent effectiveness against disease to triumph over infectious diseases.”
The question of whether immunization prevents recipients from becoming ill and from infecting others is not unique to the current pandemic.
The new variants are so infectious that being exposed to an infected individual for one second without a mask can result in COVID. (Older version-minutes/hour time frame.)
COVIDView: A Weekly Surveillance Summary of U.S. COVID-19 Activity
Updated Feb. 5, 20
Starting Friday, February 12, 2021, COVIDView will be replaced with the COVID Data Tracker Weekly Review . This new webpage and newsletter will highlight key data from CDC’s COVID Data Tracker, narrative interpretations of the data, and visualizations from the week. The new Weekly Review will also summarize important trends in the pandemic and bring together CDC data and reporting in a centralized location. It represents the extensive data that CDC uses to track the pandemic on a daily basis and will incorporate additional data sources in the future. Sign up to have the COVID Data Tracker Weekly Review delivered to your inbox every week.
(https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html)
The global effects of the coronavirus have been and will continue to be devastating for many. We knew this early on as the spread of this disease was labeled a pandemic on March 11, 2020. What areas of the economy in the US have been most affected? Today is International Women’s Day. One area only recently considered is how 10 million mothers of young children in the labor force in 2019 have been unable to return to work:
Introduction and summary
Four times as many women as men dropped out of the labor force in September, roughly 865,000 women compared with 216,000 men. This validates predictions that the impact of the COVID-19 pandemic on women—and the accompanying child care and school crises—would be severe. In July, a Washington Post article—titled, “Coronavirus child-care crisis will set women back a generation”—pointed out that “[o]ne out of four women who reported becoming unemployed during the pandemic said it was because of a lack of child care—twice the rate among men.”[1]
Another area which is truly shocking is the total death toll of the current pandemic. Should the current pandemic be compared to the Spanish influenza pandemic of 1918? The current coronavirus pandemic has resulted in worldwide devastation and will undoubtedly affect many for years to come:
History of 1918 Flu Pandemic
The 1918 influenza pandemic was the most severe pandemic in recent history. It was caused by an H1N1 virus with genes of avian origin. Although there is not universal consensus regarding where the virus originated, it spread worldwide during 1918-1919. In the United States, it was first identified in military personnel in spring 1918.
It is estimated that about 500 million people or one-third of the world’s population became infected with this virus. The number of deaths was estimated to be at least 50 million worldwide with about 675,000 occurring in the United States. Mortality was high in people younger than 5 years old, 20-40 years old, and 65 years and older. The high mortality in healthy people, including those in the 20-40 year age group, was a unique feature of this pandemic. https://www.cdc.gov/flu/pandemic-resources/1918-commemoration/1918-pandemic-history.htm
Why do I mention this prior pandemic of 100 years ago? Has general reporting of the severity been accurate, or to the estimation of many epidemiologists overly sensationalized and misrepresented? It is appropriate to recognize that in the “land of the free and home of the brave” we have little control over taking the personal responsibility of protecting ourselves, family, friends and general public from contracting and spreading this virus when government oversteps it prescribed bounds. Our Constitution openly and directly prohibits state and federal government from interfering with personal liberties like speech, press, travel, assembly, religion and commerce. At times it seems an overbearing government, without public debate, purports to be acting in the name of public safety while disregarding many of the freedom-protecting clauses of our Constitution. Consider that a personal observation.
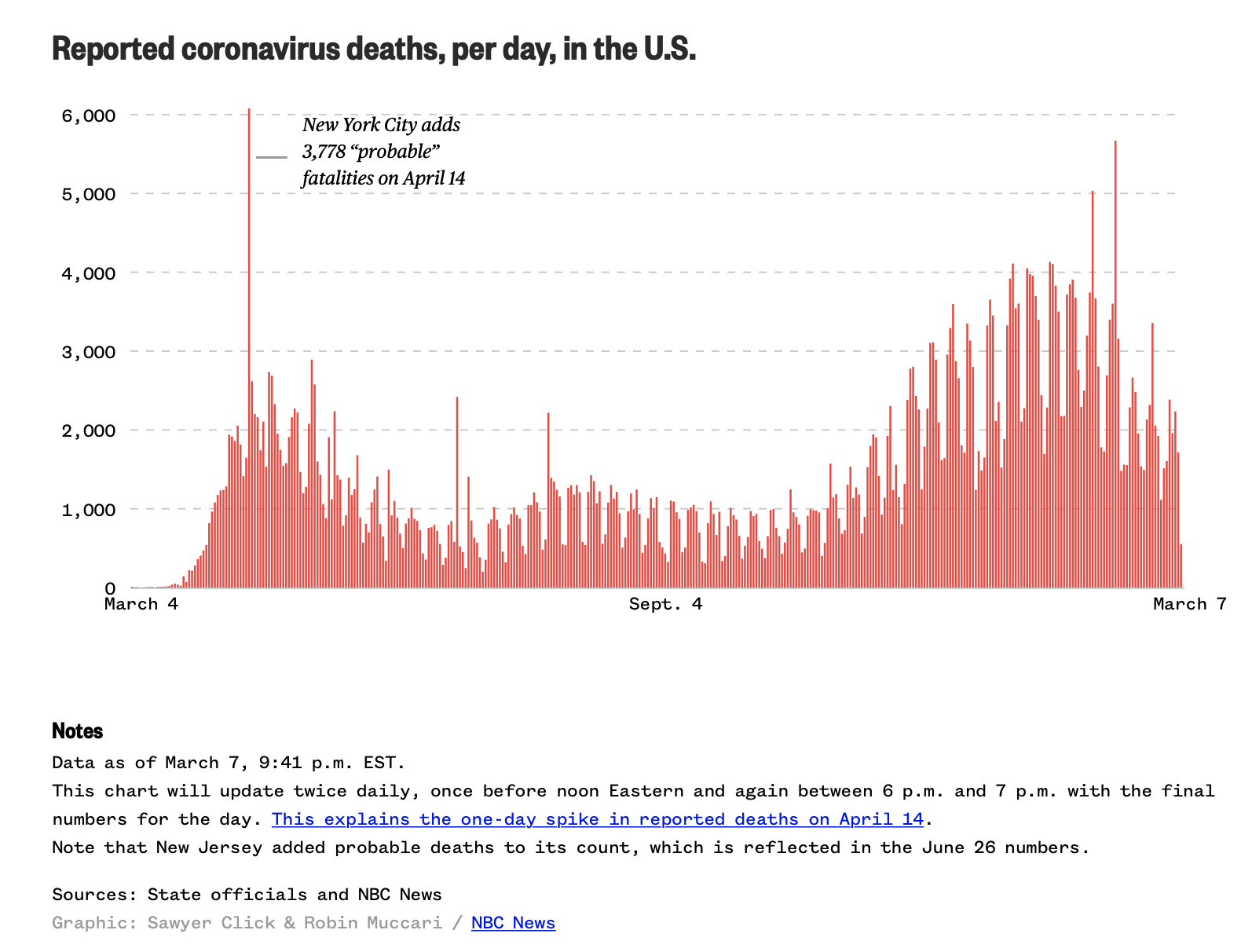
What I wanted to show in the following graph is not necessarily how devastating the death toll has been, because the death toll of Covid19 coronavirus has been very great. It is not, however, very comparable to the death toll of the Spanish influenza pandemic of 1918. Why is this not an accurate comparison? Note that the population in 1918 was less than 1/3 of the population of the U.S. today. It is estimated the Spanish flu resulted in the death of approximately 0.5% of the population in the U.S., but how great is that total deathrate if it were applied to today’s population? Assuming 330M, a 0.5% deathrate total would result in 1.65M deaths. Thankfully, modern therapeutics and medical practices, and now multiple vaccines have mitigated the severity of what the possible death toll could have been. It is still largely up to the individual to take all appropriate measures to protect themselves and others commensurate with risk factors specific to their own age, health and geographic region. The government does have a role, but it should be supportive while respecting the constraints of the Constitution, IMO.
The thing I notice from the above graphic representation is the 3 hardest hit states in the spring of 2020 were New Jersey, New York and Massachusetts, which along with Conneticut make up the vast majority of total deaths in the country during the early months. The recent alarmingly large number of deaths in late fall of 2020 and early winter 2021 are from all 50 states. One should consider this when looking and comparing these time periods. Recent data includes a much larger population of affected individuals.
Yesterday morning I learned that “word of mouth” is actually the best way to get the vaccine. I was told by a friend that the local Wal-Mart had ”no show” vaccines left over at end of the day and that they’ll distribute on a first come basis. I showed up at 4:30 PM in the afternoon and received the vaccination and a schedule to return in three weeks. That alone tells me it was the PFE vaccine (as opposed to returning in 4 weeks for the Moderna vaccine). Instead of a big scary needle as used on TV, I was effortless vaccinated through a self-closing Band-Aid with a 25 gauge needle. I didn’t even feel it! Now, after the better part of a day, I’m a little warm with a slight ache in the muscle, but that’s all I have to report for now. Thank God for good friends. Glad the vaccine after effects for me, so far, are not as bad as I’ve heard it could be for many.
I had also talked to a friend the day before up in the D.C. area and was told even though he signed up, and he is qualified to receive the Covid19 vaccine, he has not had a call back to be put on the vaccination schedule. I reported to him that here in Vancouver WA the distribution back up is very much the same. I’m signed up and qualified, but schedules are a full two months out with no vacancies. I had no success in getting scheduled. There are about 20 “official” sites for vaccinations to check on here, but none seem to have vacancies, and inquiries are met with “check back daily”. It was later a local friend had informed me of Wal-Mart’s end of day distributions here locally. Perhaps one of you reading this will find vaccine availability in your area through unconventional “word of mouth” sources if you have been frustrated from unavailability on official sites.
Updated from a posting a year ago…
** People Who Are Sick, Or Died From Co-vid??
Maybe a simple tally. From Boots on the ground. #1. Know anybody that has had the virus? #2. If yes…
A. did they survive it? or
B. Died from it?
Feel free to add any notes on either A. or B. They will be kindly read.
Such as; If they survived, how? Hospitalized? Or at Home? And how are the fairing now? Fully recovered?
Or if died;
Was it from the virus alone? … or had been immune compromised before coming down with the virus.
Nov 2019**
A. 1 person= Survived. I know of one victim so far. Male: 68 . #1. (That First person)Came down with it in Thailand. Mid Nov. 2019
. Two weeks of flue like symptoms.Quarantined and recovered in place near his Hotel room. Recovered to what he considers his normal health. Side note He also has Parkinson’s disease. …
(updated to now Mar 8-2021) I know of 11 who have tested positive. All have been USA persons, all are still alive, one has complications from having had the virus, now has diabetes problems which he never had before.
No deaths that I have heard from. *local VA cemetery has about same amount of new graves as years before. And there are a lot of old veterans still around.
So Stay healthy, get outside and enjoy nature and others. Be honest in what “you” read and think" for yourself.
Doctor Copper: this Canadian mining company explains how the red metal fights COVID-19
The COVID-19 virus survives for less than four hours on copper surfaces, compared to up to three days on plastic and stainless steel.
The use of copper in the physical environment of both healthcare and everyday high-touch settings can complement other measures to combat the spread of diseases.
For more than 10,000 years, copper has played numerous critical roles in human civilization. The red metal’s pliability, conductivity and durability have seen it used in everything from early tools to plumbing to modern electronics. In fact, copper is now so ubiquitous that the health of the copper market is often a predictor of the health of the economy overall – a fact that’s earned it the nickname “Doctor Copper”.
Today, as the world grapples with a pandemic, it turns out that the Doctor has an important part to play in healthcare, thanks to an unusual property that makes the metal a coronavirus killer. Copper is naturally anti-microbial, eliminating up to 99.9% of harmful bacteria and viruses by “punching holes in the microorganisms,” according to Dr Titus Wong, Regional Medical Director of Infection Control at Vancouver Coastal Health.
A recent study from the US National Institutes of Health, Center for Disease Control, UCLA and Princeton University scientists found that the COVID-19 virus survived for less than four hours on copper surfaces, compared to up to three days on plastic and stainless steel. And a new Vancouver Coastal Health study, confirmed copper’s durability and infection control benefits in a hospital setting. The study highlights the effectiveness of using copper to kill unwanted bacteria and viruses, demonstrating that its use in products and surfaces can help combat the spread of diseases such as COVID-19.
When placed on an antimicrobial surface, E. coli O157:H7 dies off slowly at first, then succumbs rapidly.
That research is part of the Copper & Health programme that Teck Resources has been working on in cooperation with healthcare professionals and partners in academia since 2016. The goal of the programme is to assess copper’s potential to make communities safer by reducing healthcare-acquired infections (HAIs). HAIs are the fourth-leading cause of death in Canada, costing the healthcare system more than $1 billion annually. According to York Health Economics Consortium, the cost of installing antimicrobial copper can be recouped in less than two months as a result of savings found through a significant reduction in patient infections and reduced length of hospital stay.
Copper has already been installed on high-touch surfaces such as doorknobs, counters, bedrails, light switches, and railings across more than 300 healthcare facilities in 26 countries. Through Copper & Health, Teck Resources has supported increased awareness and research on copper’s antimicrobial use in Canada, as well as pilot projects to test it in healthcare settings. This includes the installation of copper-infused countertops in Vancouver General Hospital – the first such use of copper in a Canadian hospital.
As the current global pandemic has made clear, sanitizing surfaces is critical not just in hospitals, but in all high traffic areas. In Santiago, Chile, ten kilometers of copper-alloy handrails have already been installed along the subway lines, with plans to add more copper surfaces throughout the transit system.
A car plant in Ontario recently installed copper-coated handrails as part of COVID-19 prevention measures prior to restarting. Copper surfaces are also appearing in training centres for professional sports teams, in airports and in restaurants, where uses range from exercise equipment to elevator buttons to kitchen appliances.
While this progress is promising, the adoption of copper for infection is still in the very early stages. As a major copper producer with an abundance of mineral resources and mining expertise, Canada can help lead a global shift towards the use of copper surfaces both in healthcare, as well as everyday settings, to help save lives.
Of course, the most effective means to combat COVID-19, or any other virus, remain frequent handwashing, good hygiene and physical distancing. But the strategic use of copper can supplement these, to make the physical environment actively fight back against harmful bacteria and viruses.
** As I remember, we have a little copper in those mountains also..$ C.s.
Grimm,
Are you complaining or complimenting me at insights I (& others here) care to share? I appreciate those who actually contribute information or offer intelligible comments to this forum. Would you care to tell me again exactly what you think I was saying? I think you may have mistaken the purpose of this forum.
2020 was far too strange and stressful a year for most of us. Far more were saved than died, not because of the devotion of politicians, but from the hard work by those who put forth their knowledge and expertise to find a way to combat the disease. Thank God, and the multitude of scientists and healthcare workers that devoted their time and energy to this effort. There were many incremental advances along the way. As the best policies were being adopted to lessen the overall impact of this pandemic, some individual states did much better than others, despite political interference and obstruction. Some of the same measures that are used in all pandemics (recall the Spanish Flu pandemic) were useful, but it was the science and modern technology that lessened the toll of this pandemic in the US. It is inevitable many deaths will result from a virulent virus that causes a worldwide pandemic. I give much credit to those who actually look at and present the facts, and then come up with solutions. It was back in October I posted:
Focused Protection and individual responsibility are the best ways to fight this devastating pandemic, along with all the modern therapeutics and vaccines developed for this coronavirus. Here it is again, incase you missed it. It should not have been controversial as it is proving to be the entirely right approach:
The Great Barrington Declaration
The Great Barrington Declaration – As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.
Coming from both the left and right, and around the world, we have devoted our careers to protecting people. Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimize mortality and social harm until we reach herd immunity.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
Adopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent testing of other staff and all visitors. Staff rotation should be minimized. Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.
On October 4, 2020, this declaration was authored and signed in Great Barrington, United States, by:
Dr. Martin Kulldorff , professor of medicine at Harvard University, a biostatistician, and epidemiologist with expertise in detecting and monitoring infectious disease outbreaks and vaccine safety evaluations.
Dr. Sunetra Gupta , professor at Oxford University, an epidemiologist with expertise in immunology, vaccine development, and mathematical modeling of infectious diseases.
Dr. Jay Bhattacharya , professor at Stanford University Medical School, a physician, epidemiologist, health economist, and public health policy expert focusing on infectious diseases and vulnerable populations. https://gbdeclaration.org
Nice contribution CS. When I think of a metal that has antimicrobial properties I usually think of silver. I’m looking at silver a lot more these days, but not for medicinal purposes.
I knew copper and copper paint was useful on boat hulls, but hadn’t really thought of it’s antimicrobial properties until you mentioned it.
Copper and its alloys (brasses, bronzes, cupronickel, copper-nickel-zinc, and others) are natural antimicrobial materials. Ancient civilizations exploited the antimicrobial properties of copper long before the concept of microbes became understood in the nineteenth century.[1][2][3] In addition to several copper medicinal preparations, it was also observed centuries ago that water contained in copper vessels or transported in copper conveyance systems was of better quality (i.e., no or little visible slime or biofouling formation) than water contained or transported in other materials.[ citation needed ]
The antimicrobial properties of copper are still under active investigation. Molecular mechanisms responsible for the antibacterial action of copper have been a subject of intensive research. Scientists are also actively demonstrating the intrinsic efficacy of copper alloy “touch surfaces” to destroy a wide range ofmicroorganisms that threaten public health.[4]
It’s not just the death rate I was worried about, it’s the side affects to those who only get mild cases of it. I have a friend in her early 50’s who got it. Didn’t need to go to hospital, but she’s now a “longhauler” as she’s still affected by symptoms of it 6 months after it. One of my daughters works in public health and she was telling me they’re finding lung damage in younger people that showed no signs of having it, but have the antibodies in their blood from having it. FWIW
Your daughter is so right on this. Otherwise healthy younger individuals without comorbidities are experiencing a number of effects from mild to more severe even after the active disease is gone. MG commentented on this quite a lot earlier in the thread. There were many main concerns early on, but most public health officials were concerned with rising mortality figures and implementing policies to keep hospitals from overreaching capacity. Here is just one such article from early on that was written concerning this topic, and there are many:
Post-Covid-19 rehab for athletes: start with pulmonary function
Knowing that responses to the virus are unpredictable, the chances are still high that athletes who fall ill with the coronavirus will need rehabilitation to return to sport. The coronavirus attacks all bodily systems, but primarily affects the lower respiratory tract. While the disease process presents with a variety of symptoms, including fatigue, sore throat, fever, diarrhea, and vomiting, shortness of breath is the hallmark complaint. The compromise that occurs in the lungs during the active disease may have lasting effects after the patient gets well.
Doctors in Hong Kong recently (March 13, 2020) reported the findings of the first follow-up clinics of recovered Covid-19 patients(1). They suppose that some recovered patients have lost between 20% to 30% of their previous lung function(1). These reports come after a review of a small population, about a dozen or so patients, of which around one-quarter had shortness of breath during functional activities despite disease resolution. The doctors report that lung scans of recovered patients also reveal substantial lung damage. There was no mention as to whether these patients were previously mechanically ventilated or not. Sports Injury Bulletin - Email Newsletters - Post-Covid-19 rehab for athletes: start with pulmonary function
Here is a more recent one:
Long-term Effects of COVID-19 in Athletes
In earlier stages of the pandemic, much attention was focused on acute respiratory complications which increase the risk of mortality and morbidity. However, attention is now turning towards the impact that COVID-19 exerts on the cardiovascular system.
A small, but growing body of research suggests that the disease may exacerbate heart failure in patients with established cardiac conditions. Patients with acute COVID-19 have demonstrated elevated levels of troponin, a protein that is released when the heart muscle becomes damaged, in the bloodstream. Long-term Effects of COVID-19 in Athletes
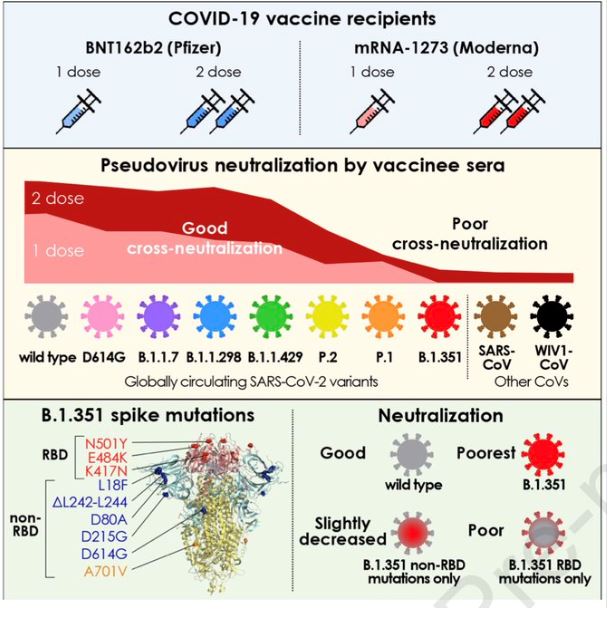
The top 2 vaccines in U.S. are not protective against 2 of the new variants(S. African variant in particular) per latest study. Although these 2 variants are still rare in the U.S., its only a matter of time before they spread especially since the current case load remains very high and has begun to trend higher once again.
Note that 70 million American’s ages 0 to 16 will not even be eligible for a vaccine till the Fall at the earliest. Note also that 47% of republicans have indicated that they have no plans to be vaccinated and it is easy to guess that 2021 won’t be the year that we see the end of the pandemic. All of these unvaccinated people both here and abroad will also simply provide more of a breeding ground for new variants to develop and spread. Sure new vaccines are being developed but they are already behind the curve.