A rather long article appearing in the Washington Post outlining some recent revelations in research of the coronavirus (there are imbedded video clips in the article - check the link out to view the clips):
Forty percent of people with coronavirus infections have no symptoms. Might they be the key to ending the pandemic?
New research suggests that some of us may be partially protected due to past encounters with common cold coronaviruses.
By
Ariana Eunjung Cha
August 8, 2020 at 10:31 a.m. PDT
When researcher Monica Gandhi began digging deeper into outbreaks of the novel coronavirus, she was struck by the extraordinarily high number of infected people who had no symptoms.
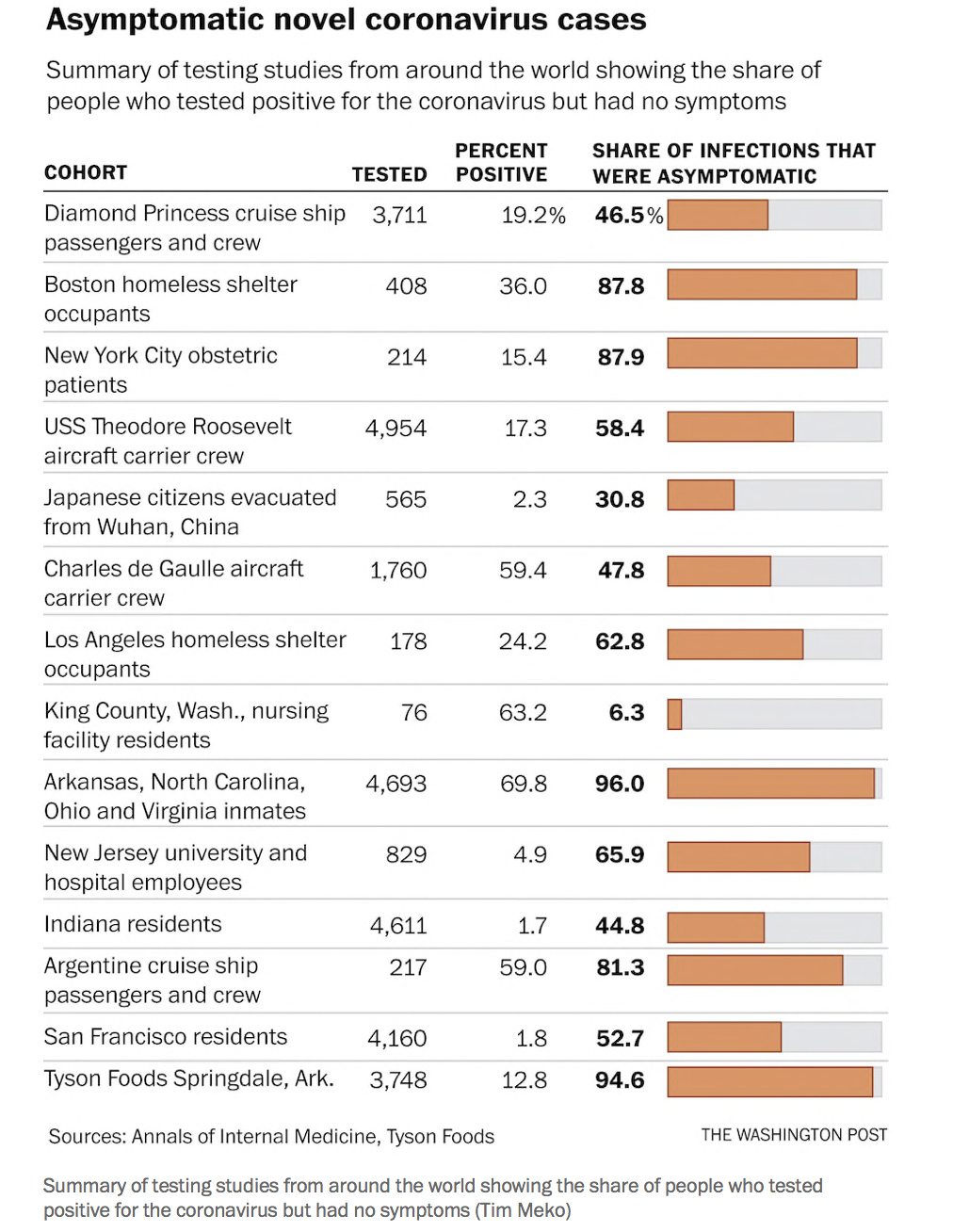
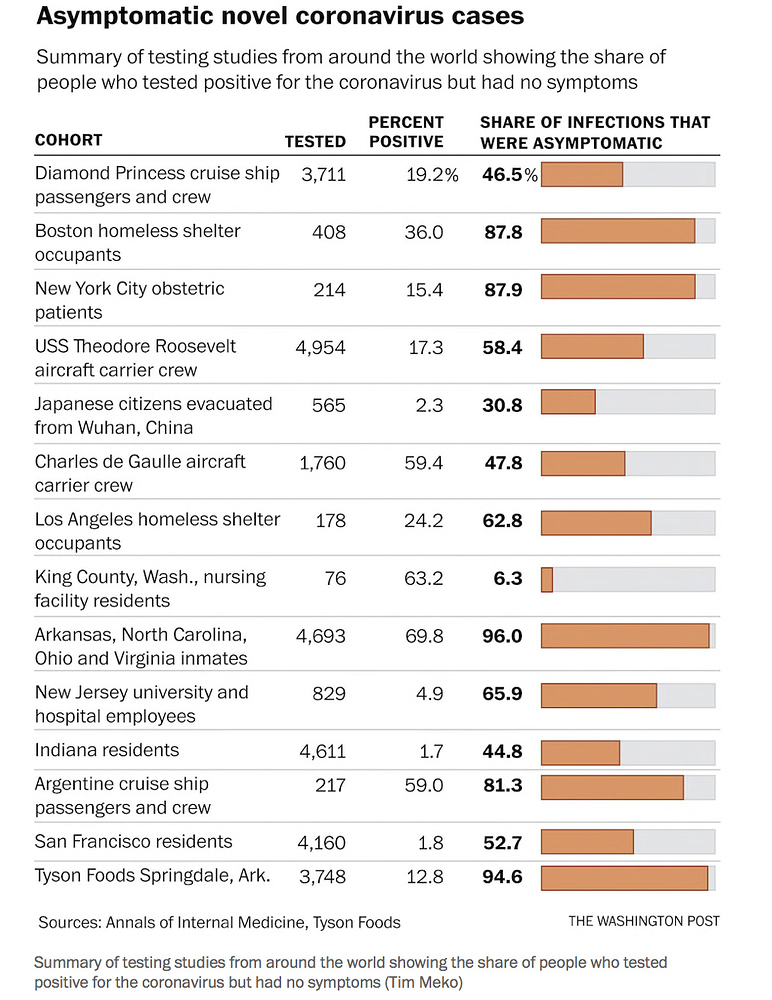
A Boston homeless shelter had 147 infected residents, but 88 percent had no symptoms even though they shared their living space. A Tyson Foods poultry plant in Springdale, Ark., had 481 infections, and 95 percent were asymptomatic. Prisons in Arkansas, North Carolina, Ohio and Virginia counted 3,277 infected people, but 96 percent were asymptomatic.
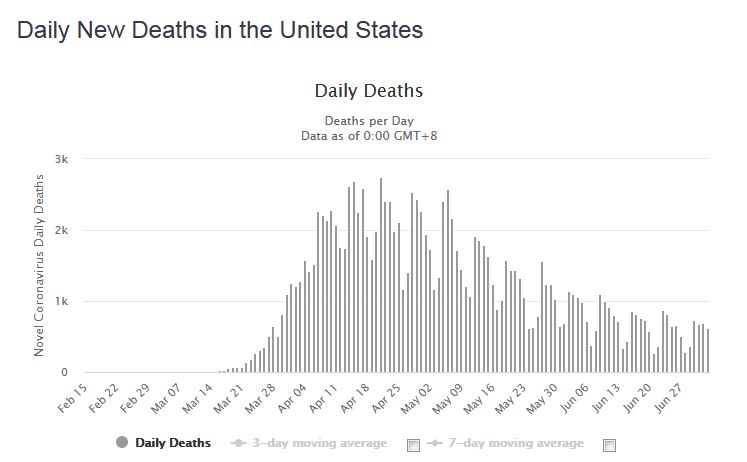
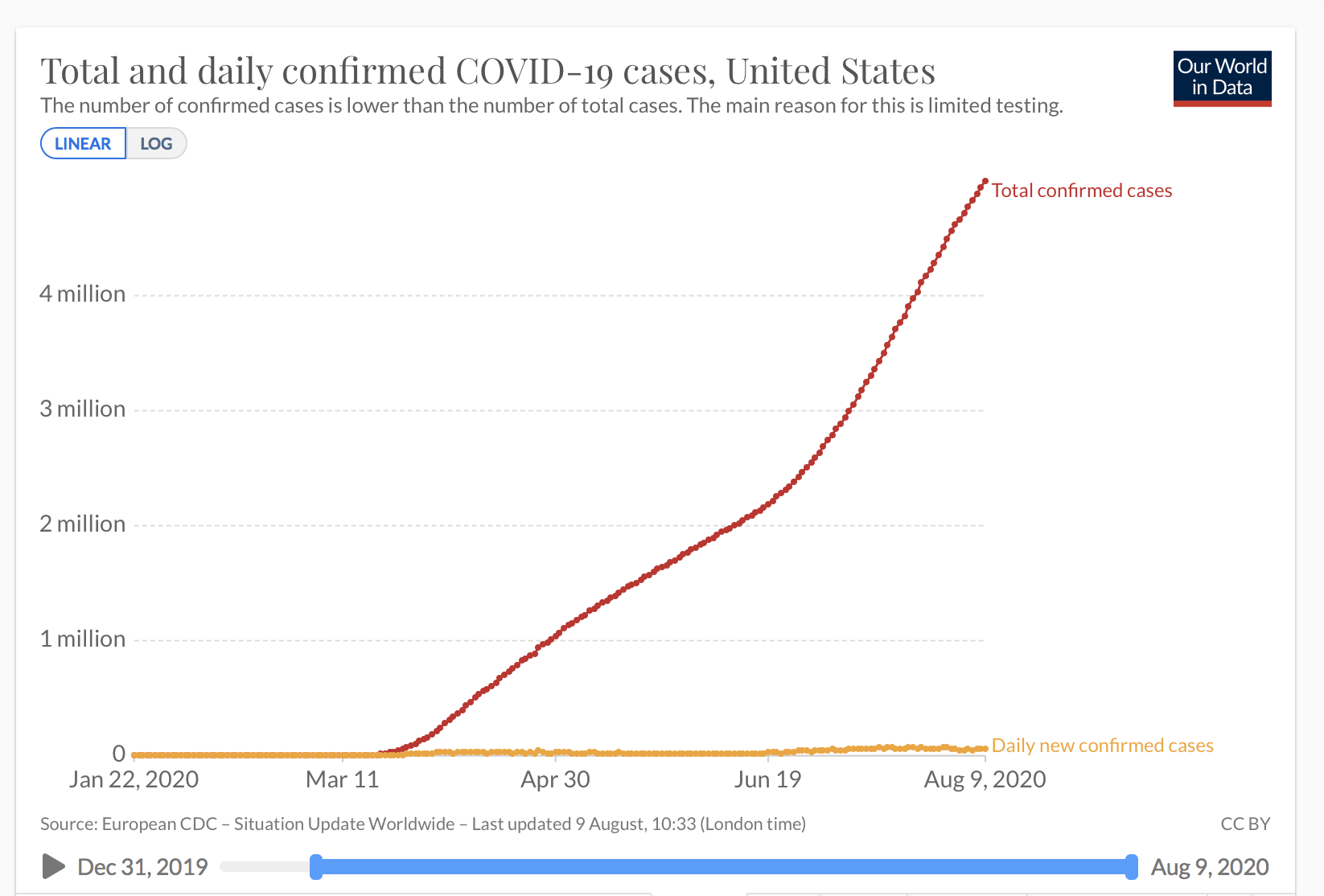
During its seven-month global rampage, the coronavirus has claimed more than 700,000 lives. But Gandhi began to think the bigger mystery might be why it has left so many more practically unscathed.
What was it about these asymptomatic people, who lived or worked so closely to others who fell severely ill, she wondered, that protected them? Did the “dose” of their viral exposure make a difference? Was it genetics? Or might some people already have partial resistance to the virus, contrary to our initial understanding?
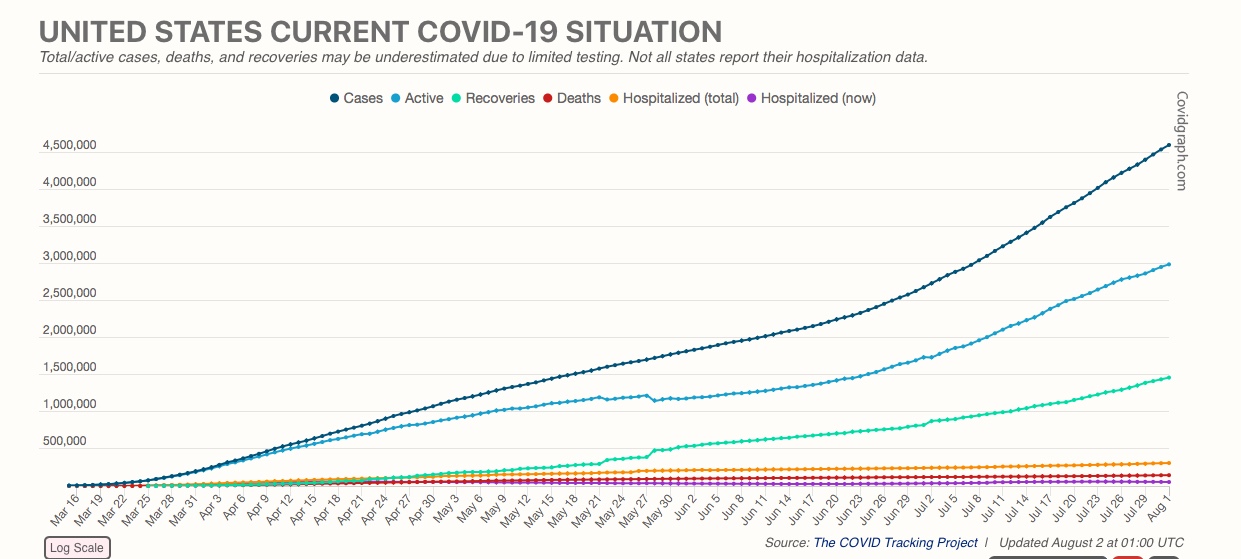
U.S. coronavirus map: Tracking cases and deaths
Efforts to understand the diversity in the illness are finally beginning to yield results, raising hope the knowledge will help accelerate development of vaccines and therapies — or possibly even create new pathways toward herd immunity in which enough of the population develops a mild version of the virus that they block further spread and the pandemic ends.
“A high rate of asymptomatic infection is a good thing,” said Gandhi, an infectious-disease specialist at the University of California at San Francisco. “It’s a good thing for the individual and a good thing for society.”
The coronavirus has left numerous clues — the uneven transmission in different parts of the world, the mostly mild impact on children. Perhaps most tantalizing is the unusually large proportion of infected people with no symptoms. The Centers for Disease Control and Prevention last month estimated that rate at about 40 percent.
Those clues have sent scientists off in different directions: Some are looking into the role of the receptor cells, which the virus uses to infiltrate the body, to better understand the role that age and genetics might play. Others are delving into face masks and whether they may filter just enough of the virus so that those wearing them had mild cases or no symptoms at all.
The theory that has generated the most excitement in recent weeks is that some people walking among us might already have partial immunity.
One mind-blowing hypothesis — bolstered by a flurry of recent studies — is that a segment of the world’s population may have partial protection thanks to “memory” T cells, the part of our immune system trained to recognize specific invaders. This could originate from cross protection derived from standard childhood vaccinations. Or, as a paper published Tuesday in Science suggested, it could trace back to previous encounters with other coronaviruses, such as those that cause the common cold.
“This might potentially explain why some people seem to fend off the virus and may be less susceptible to becoming severely ill,” National Institutes of Health Director Francis Collins remarked in a blog post this past week.
On a population level, such findings, if validated, could be far-reaching.
Hans-Gustaf Ljunggren, a researcher at Sweden’s Karolinska Institute, and others have suggested that public immunity to the coronavirus could be significantly higher than what has been suggested by serology studies. In communities in Boston, Barcelona, Wuhan and other major cities, the proportion of people estimated to have antibodies and therefore presumably be immune has mostly been in the single digits. But if others had partial protection from T cells, that would raise a community’s immunity level much higher.
This, Ljunggren said, would be “very good news from a public health perspective.”
Asked and answered: What readers want to know about coronavirus
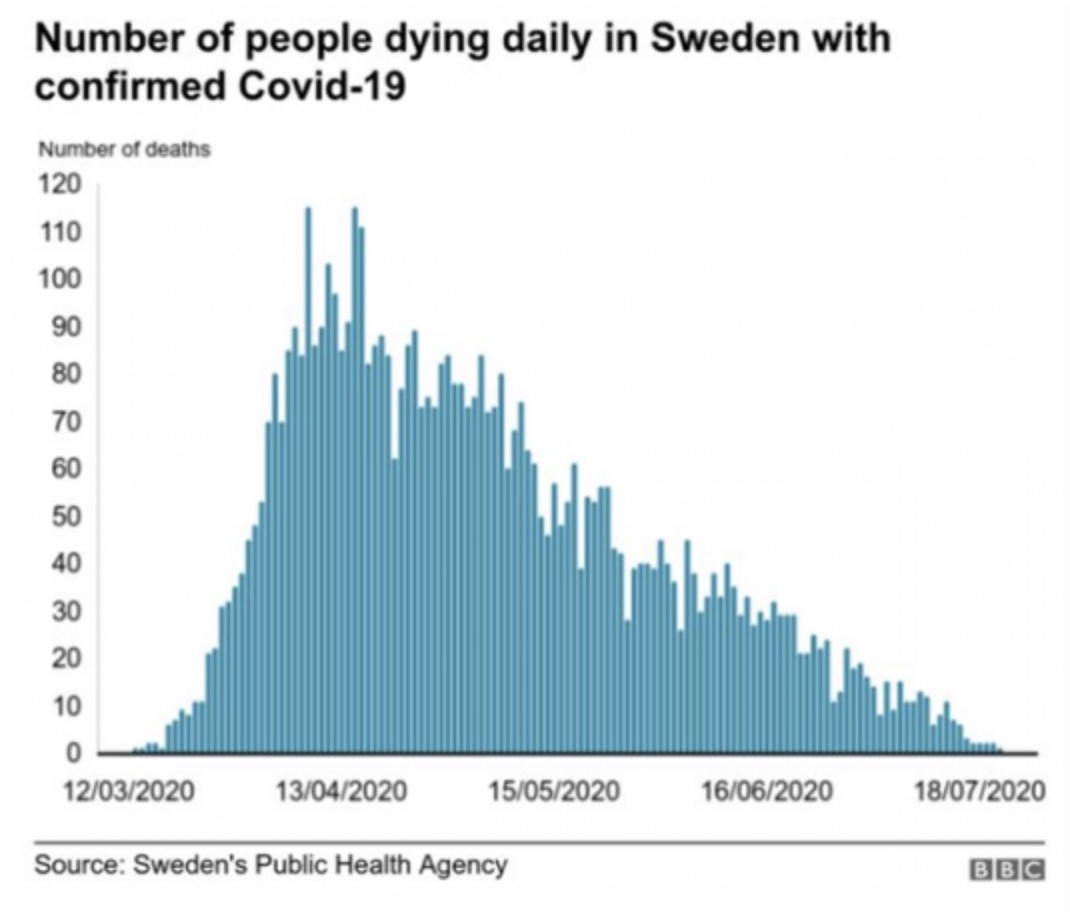
Some experts have gone so far as to speculate whether some surprising recent trends in the epidemiology of the coronavirus — the drop in infection rates in Sweden where there have been no widespread lockdowns or mask requirements, or the high rates of infection in Mumbai’s poor areas but little serious disease — might be due to preexisting immunity.
Others say it’s far too early to draw such conclusions. Anthony S. Fauci, the United States’ top infectious-disease expert, said in an interview that while these ideas are being intensely studied, such theories are premature. He agreed that at least some partial preexisting immunity in some individuals seems a possibility.
Fauci explains phase 3 of vaccine trial, shows optimism for vaccine in late 2020
Anthony S. Fauci, the nation’s top infectious disease expert, explains the next phase to involving 30,000 volunteers to create a coronavirus vaccine. (Reuters)
And he said the amount of virus someone is exposed to — called the inoculum — “is almost certainly an important and likely factor” based on what we know about other viruses.
But Fauci cautioned there are multiple likely reasons — including youth and general health — that determine whether a particular individual shrugs off the disease or dies of it. He also emphasized that even those with mild illness may have lingering medical issues.
That reinforces the need, in his view, for continued vigilance in social distancing, masking and other precautions.
“There are so many other unknown factors that maybe determine why someone gets an asymptomatic infection,” Fauci said. “It’s a very difficult problem to pinpoint one thing.”
Immune memory machine
France’s President Emmanuel Macron talks last month in Brussels with German Chancellor Angela Merkel, Finland’s Prime Minister Sanna Marin and Sweden’s Prime Minister Stefan Lofven in their first face-to-face summit since the coronavirus outbreak. (John Thys/Pool/Reuters)
France’s President Emmanuel Macron talks last month in Brussels with German Chancellor Angela Merkel, Finland’s Prime Minister Sanna Marin and Sweden’s Prime Minister Stefan Lofven in their first face-to-face summit since the coronavirus outbreak. (John Thys/Pool/Reuters)
News headlines have touted the idea based on blood tests that 20 percent of some New York communities might be immune, 7.3 percent in Stockholm, 7.1 percent in Barcelona. Those numbers come from looking at antibodies in people’s blood that typically develop after they are exposed to a virus. But scientists believe another part of our immune system — T cells, a type of white blood cell that orchestrates the entire immune system — could be even more important in fighting against the coronavirus.
Recent studies have suggested that antibodies from the coronavirus seem to stick around for only two to three months in some people. While work on T cells and the coronavirus is only getting started — testing T cells is much more laborious than antibody testing — previous research has shown that, in general, T cells tend to last years longer.
One of the first peer-reviewed studies on the coronavirus and T cells was published in mid-May in the journal Cell by Alessandro Sette, Shane Crotty and others at the La Jolla Institute for Immunology near San Diego.
The group was researching blood from people who were recovering from coronavirus infections and wanted to compare that to samples from uninfected controls who were donors to a blood bank from 2015 to 2018. The researchers were floored to find that in 40 to 60 percent of the old samples, the T cells seemed to recognize SARS-CoV-2.
“The virus didn’t even exist back then, so to have this immune response was remarkable,” Sette said.
Research teams from five other locations reported similar findings. In a study from the Netherlands, T cells reacted to the virus in 20 percent of the samples. In Germany, 34 percent. In Singapore, 50 percent.
The different teams hypothesized this could be due to previous exposure to similar pathogens. Perhaps fortuitously, SARS-CoV-2 is part of a large family of viruses. Two of them — SARS and MERS — are deadly and led to relatively brief and contained outbreaks. Four other coronavirus variants, which cause the common cold, circulate widely each year but typically result in only mild symptoms. Sette calls them the “less-evil cousins of SARS-CoV-2.”
This week, Sette and others from the team reported new research in Science providing evidence the T cell responses may derive in part from memory of “common cold” coronaviruses.
“The immune system is basically a memory machine,” he said. “It remembers and fights back stronger.”
Interestingly, the researchers noted in their paper, the strongest reaction they saw was against the spike proteins that the virus uses to gain access to cells — suggesting that fewer viral copies get past these defenses.
“The current model assumes you are either protected or you are not — that it’s a yes or no thing,” Sette added. “But if some people have some level of preexisting immunity, that may suggest it’s not a switch but more continuous.”
Childhood vaccines
A scientific illustration of the SARS-CoV-2 coronavirus binding to a receptor on a human cell. This attachment is the initial step in the development of a coronavirus infection. (Kateryna Kon/Science Photo/Getty Images)
A scientific illustration of the SARS-CoV-2 coronavirus binding to a receptor on a human cell. This attachment is the initial step in the development of a coronavirus infection. (Kateryna Kon/Science Photo/Getty Images)
Nearly 2,000 miles away, at the Mayo Clinic in Rochester, Minn., Andrew Badley was zeroing in the possible protective effects of vaccines.
Teaming up with data experts from nference, a company that manages their clinical data, he and other scientists looked at records from 137,037 patients treated at the health system to look for relationships between vaccinations and coronavirus infection.
They knew that the vaccine for smallpox, for example, had been shown to protect against measles and whooping cough. Today, a number of existing vaccines are being studied to see if any might offer cross-protection against SARS-CoV-2.
The results were intriguing: Seven types of vaccines given one, two or five years in the past were associated with having a lower rate of infection with the new coronavirus. Two vaccines in particular seemed to show stronger links: People who got a pneumonia vaccine in the recent past appeared to have a 28 percent reduction in coronavirus risk. Those who got polio vaccines had a 43 percent reduction in risk.
Venky Soundararajan, chief scientific officer of nference, remembers when he first saw how large the reduction appeared to be, he immediately picked up his phone and called Badley: “I said, ‘Is this even possible?’”
The team looked at dozens of other possible explanations for the difference. They adjusted for geographic incidence of the coronavirus, demographics, comorbidities, even whether people had had mammograms or colonoscopies under the assumption that people who got preventive care might be more apt to social distance. But the risk reduction still remained large.
“This surprised us completely,” Soundararajan recalled. “Going in we didn’t expect anything or maybe one or two vaccines showing modest levels of protection.”
The study is only observational and cannot show a causal link by design, but Mayo researchers are looking at a way to quantify the activity of these vaccines on the coronavirus to serve as a benchmark to the new vaccines being created by companies such as Moderna. If existing vaccines appear as protective as new ones under development, he said, they could change the world’s whole vaccine strategy.
A vaccine, or millions of deaths: How America can build herd immunity to the coronavirus
Genetics and biology
The novel coronavirus uses a number of tools to infect our cells and replicate. What we’ve learned from SARS and MERS can help fight covid-19. (Video: Brian Monroe/Photo: Brian Monroe/The Washington Post)
The novel coronavirus is a master of disguise: Here’s how it works
The novel coronavirus uses a number of tools to infect our cells and replicate. What we’ve learned from SARS and MERS can help fight covid-19. (Video: Brian Monroe/Photo: Brian Monroe/The Washington Post)
At NIH headquarters in Bethesda, Md., meanwhile, Alkis Togias has been laser-focused on one group of the mildly impacted: children. He wondered if it might have something to do with the receptor known as ACE2, through which the virus hitchhikes into the body.
In healthy people, the ACE2 receptors perform the important function of keeping blood pressure stable. The novel coronavirus latches itself to ACE2, where it replicates. Pharmaceutical companies are trying to figure out how to minimize the receptors or to trick the virus into attaching itself to a drug so it doesn’t replicate and travel throughout the body.
Was it possible, Togias asked, that children naturally expressed the receptor in a way that makes them less vulnerable to infection?
He said recent papers have produced counterintuitive findings about one subgroup of children — those with a lot of allergies and asthma. The ACE2 receptors in those children were diminished, and when they were exposed to an allergen such as cat hair, the receptors were further reduced. Those findings, combined with data from hospitals showing that asthma did not seem to be a risk factor for the respiratory virus, as expected, have intrigued researchers.
“We are thinking allergic reactions may protect you by down-regulating the receptor,” he said. “It’s only a theory of course.”
Togias, who is in charge of airway biology for the National Institute of Allergy and Infectious Diseases, is looking at how those receptors seem to be expressed differently as people age, as part of a study of 2,000 U.S. families. By comparing those differences and immune responses within families, they hope to be able to better understand the receptors’ role.
Separately, a number of genetic studies show variations in genes associated with ACE2 with people from certain geographic areas, such as Italy and parts of Asia, having distinct mutations. No one knows what significance, if any, these differences have on infection, but it’s an active area of discussion in the scientific community.
Masks
A passenger in quarantine February on the Diamond Princess cruise ship in Yokohama, Japan. (Takashi Aoyama/Getty Images)
A passenger in quarantine February on the Diamond Princess cruise ship in Yokohama, Japan. (Takashi Aoyama/Getty Images)
Before the pandemic, Gandhi, the University of California researcher, specialized in HIV. But like other infectious-disease experts these days, she has spent many of her waking hours thinking about the coronavirus. And in scrutinizing the data on outbreaks one day, she noticed what might be a pattern: People were wearing masks in the settings with the highest percentage of asymptomatic cases.
The numbers on two cruise ships were especially striking. In the Diamond Princess, where masks weren’t used and the virus was likely to have roamed free, 47 percent of those tested were asymptomatic. But in the Antarctic-bound Argentine cruise ship, where an outbreak hit in mid-March and surgical masks were given to all passengers and N95 masks to the crew, 81 percent were asymptomatic.
Similarly high rates of asymptomatic infection were documented at a pediatric dialysis unit in Indiana, a seafood plant in Oregon and a hair salon in Missouri, all of which used masks. Gandhi was also intrigued by countries such as Singapore, Vietnam and the Czech Republic that had population-level masking.
“They got cases,” she noted, “but fewer deaths.”
The scientific literature on viral dose goes back to around 1938 when scientists began to find evidence that being exposed to one copy of a virus is more easily overcome than being exposed to a billion copies. Researchers refer to the infectious dose as ID50 — or the dose at which 50 percent of the population would become infected.
While we don’t know what that level might be for the coronavirus (it would be unethical to expose humans in this way), previous work on other nonlethal viruses showed that people tend to get less sick with lower doses and more sick with higher doses. A study published in late May involving hamsters, masks and SARS-CoV-2 found those given coverings had milder cases than those who did not get them.
In an article published this month in the Journal of General Internal Medicine, Gandhi noted that in some outbreaks early in the pandemic in which most people did not wear masks, 15 percent of the infected were asymptomatic. But later on, when people began wearing masks, the rate of asymptomatic people was 40 to 45 percent.
She said the evidence points to masks not just protecting others — as U.S. health officials emphasize — but protecting the wearer as well. Gandhi makes the controversial argument that while we’ve mostly talked about asymptomatic infections as terrifying due to how people can spread the virus unwittingly, it could end up being a good thing.
“It is an intriguing hypothesis that asymptomatic infection triggering immunity may lead us to get more population-level immunity,” Gandhi said. “That itself will limit spread.”
https://www.washingtonpost.com/health/2020/08/08/asymptomatic-coronavirus-covid/