Here’s something to read if you are bored this weekend and would like a little additional information. Let’s keep in mind that this thread is to discuss Global Health Effects on Markets and Mining Stock. Let’s keep it on subject by presenting useful intelligible information. In discussions it is normal to present differing views on subject matter in a courteous and responsible manner.
The thread has presented a tremendous amount of information on the virus. Keep in mind that the Covid19 virus was declared a pandemic on March 11, 2020. That’s a rather long time ago. The intitial scare of a novel virus was overwhelming. It can’t be overemphasized that as much as we are learning about the nature of this virus and how to deal with it, there is still much we don’t know. An epidemic is termed a pandemic when it is no longer localized and has spread over a very large geographic area that is also affecting a large proportion of the population. This pandemic has spread globally and has shown itself to be deadly. As disheartening as it may be, there are many direct deaths associated with this particular coronavirus. It must be dealt with.
This forum has mostly presented information and ideas on how best to deal with minimizing the spread of the virus while minimizing the number of deaths. The original goal of the mandated lockdowns was to prevent overwhelming the hospital and healthcare systems from becoming completely paralyzed by an overload of patients. After 5 months, the far reaching problems of prolonged lockdowns are beginning to take a toll on the country and the world in unacceptable ways. In the months ahead, I’m quite sure there will be discussions on not just the health effects, but also the global effects this virus is having on Markets and Mining Stocks. Michael Oliver had another dry but informative interview on Palisade radio yesterday titled “Silver Will Crush Gold”; he discusses much of his earlier work on his analysis methods in the 1st half of this 40 minute interview. About the half-way mark he discusses his view of what to expect in the short and longer term time frame for the commodities. It is a good look at what to expect in the gold and silver miners this year and next.
Switching gears a bit, this is a rather long. but well written article on India’s attempt to deal with the pandemic:
Lift lockdowns, protect the vulnerable, treat Covid like a health issue and not a disaster
24 July, 2020 8:00 am IST
Serological studies have shown that 10 times more Indians have had Covid than reported, and the death rate is 0.1%. So let’s not exaggerate, say experts.
India presents a unique opportunity for a science-based approach for handling the Covid-19 pandemic in light of new scientific evidence. The availability of excellent serological evidence based on sample surveys of large populations provides crucial information for a rational path to managing the epidemic without undue fear or panic.
A serological survey measures the fraction of the population that has Covid-specific antibodies in their blood. This provides good evidence of prior infection. Recently, the ICMR has conducted a large-scale seroprevalence study in India, which estimated that tens of millions (crores) of Indians have already had the Covid-19 infection. This finding has been verified by a serological study conducted by Thyrocare and other private labs.
This may sound like bad news, but it’s actually good news. The vast number of these infected people experienced few symptoms from the infection and did not die. The vast majority are no longer infected and are not infectious.
Since there are so many previously infected people, the Covid-19 infection fatality rate (IFR) in India implied by ICMR’s previous study is around 0.1 per cent or lower — one death per thousand infections. This is much lower than the widely reported fatality rate estimate of 2.5 per cent, which ignores the large number of unreported and uncounted cases found by the serological studies. Unreported cases must then be also counted in the denominator to estimate the true danger from the Covid-19 infection.
Lockdowns are futile
Serological surveillance is a better and more reliable technique for assessing the progress of the disease rather than crude ‘increase in number of cases’ (or ‘doubling rate’) based on case counts. Increase in the number of cases is proportional to testing intensity in a population.
Likewise, reporting crude ‘recovery rate’ is unscientific, and adds to fear psychosis by falsely exaggerating the risk perception. Both of these statistics ignore the large number of unreported cases. In a widespread disease with a proven infection fatality rate below 0.1 per cent, like Covid-19 in India, it is unscientific and futile to impose lockdowns in a bid to limit the increase in case counts.
Lockdown measures cannot permanently control the spread of the virus, as is evident from the widespread prevalence of the disease in India despite the lockdown. At best, lockdowns delay the onset of the disease to after the lockdown is lifted, rather than preventing disease altogether. Lockdowns themselves cause severe damage to both lives and livelihoods, as people delay required healthcare and lose their jobs.
Widespread pandemic is good news
As there is substantial global data and experience now available, the progress of the disease is known more clearly. It is clear that India has reached a stage where in many cities, the prevalence is in double digits (more than 10 per cent) while the countryside is relatively less exposed.
However, the best part is that the number of deaths in India due to Covid-19 infection is quite low relative to the experience of other countries. In the end, Covid-19 infections will have a relatively small effect on India’s annual death count of nearly ten million.
India’s daily burden of ischemic heart disease alone is approximately 4,000 deaths. If the lockdown is continued, it is possible that more people will die from neglected treatment of other diseases than from Covid-19 itself.
The lockdown encourages mismanagement of medical services by delaying or eliminating needed care for patients with other conditions that are not specifically Covid-19. It is a wrong and self-defeating policy to count deaths only due to Covid-19 on a day-to-day basis, while ignoring deaths and other malign outcomes from other diseases as a result of lockdowns. The daily death and health incidence data should be published for all causes and not just Covid-19, to put things into perspective.
Publicising only reported Covid-19 cases and deaths is a form of misinformation, inducing fear in the population, including in the medical community. The reported case counts present a false picture of the epidemic, greatly underestimating its true spread. In fact, the actual number of cases is tens of times higher if unreported cases are also counted.
Remember, a widespread epidemic is good news, since it implies a low infection fatality rate. So, it is better to recognize and publicize the vast number of cases that recover on their own, to rightly project the relative lethality of Covid-19 and address the disproportionate scare from the early days of the epidemic.
The approach India should take
In view of the above evidence, a liberalised Swedish approach is the best course for India. This simply means emphasising public education, individual risk-taking and responsibility. The desirable, and, perhaps, unavoidable, outcome will be slow or natural exposure of the not-so-vulnerable segment of the population, while the capacity to handle severe cases is built up.
The more vulnerable (say persons of age 60-plus and with comorbid conditions) should receive special protection, including testing, close monitoring, and perhaps isolation.
The strategy of testing and tracing all asymptomatic or mild cases in order to isolate them will now be impossible, given the widespread nature of the epidemic. Waiting in lockdown for a vaccine is also risky, as the harms from the lockdown multiply. A heroic level of ‘trace, test and isolate’ will only further stigmatise the disease as it has already done, clog institutional capacity, and increase viral load all around, including on the medical personnel and on the asymptomatic or mild cases. This will make institutions hotbeds of avoidable nosocomial viral load (i.e. hospital-acquired infections) and result in more deaths.
By contrast, a decentralised approach involving all levels of primary, secondary and tertiary medical infrastructure, like any other communicable disease, will be more suited to manage the pandemic.
The ‘trace, test and isolate’ doctrine raises significant human rights issues in terms of unequal treatment and freedom of the individual, as the tested asymptomatic or mild patients are forcibly exposed to additional viral loads on not only themselves but all around, leading to more deaths, while those untested (and hence not quarantined), develop natural immunity and live.
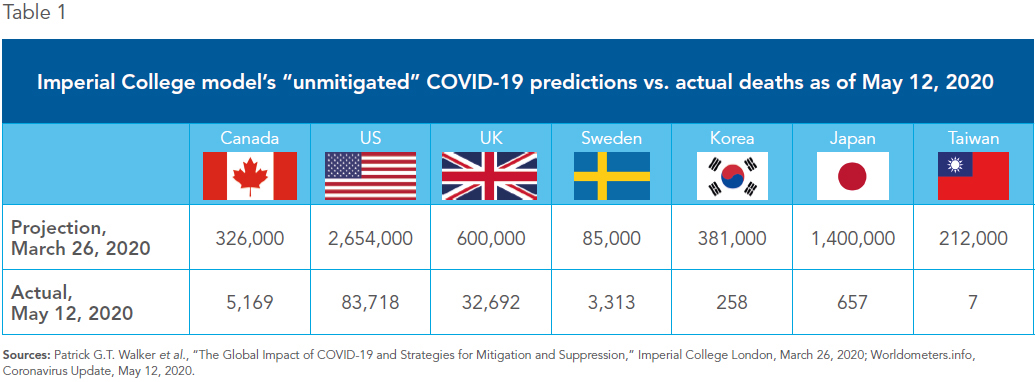
To sum up, disease projection models should be updated to account for the serological evidence of widespread disease prevalence and low infection fatality rates. Wherever the revised projection suggests that hospitals will not be overwhelmed, lockdowns must be lifted, boldly and confidently, but with special provisions to protect the vulnerable.
It is important to handle the epidemic as a public health issue and not a disaster or law and order issue. Police forces must be taken off completely, the Disaster Management Act should be lifted, and constitutional liberties fully restored. There must be a transparent disclosure of the widespread nature but very low true mortality of this disease, quite like many other diseases we live with in our day-to-day lives.
Dr Jay Bhattacharya is a professor of medicine at Stanford University, USA.
Sanjiv Agarwal is the founder of the Good Governance India Foundation, Mumbai. The GGIF is launching Rational Health Response to Covid-19, RHRC-19.com, for a collaborative response with medical practitioners in India.
This is an updated version of the letter written to PM Narendra Modi last month in response to his invitation for suggestions for Unlock 2.0.
Lift lockdowns, protect the vulnerable, treat Covid like a health issue and not a disaster