If you’ve been reading my previous posts, you may find this interesting. Instead of freaking out, overreacting and joining the global scare campaign, perhaps taking a look at the science would serve everyone better. New facts are emerging and should really be considered. Is the Omicron strain so infectious as to become the dominant strain? If so, it may be a very fortunate natural development and lead to protecting healthy individuals better than any of the vaccines! Consider the following:
Basically, in organisms with high mutations rates (such as RNA viruses), Muller’s Ratchet suggests that the mean fitness in a population will always decrease.
(virology - Muller's ratchet and viruses - Biology Stack Exchange)
Do we worry about catching the “common cold” when we are young and healthy?
Common cold
Graham Worrall, MB BS MSc FCFP
Epidemiology and symptoms
On average, adults get 4 to 6 colds per year, while children get 6 to 8 of them. Colds cause about 500 FP visits per 1000 patients per year.1 Because colds occur all year round, the total burden of illness caused by them is greater than the burden caused by seasonal influenza. Colds account for 40% of all time lost from jobs and 30% of all absenteeism from school.2 There are more than 200 viruses, continuously changing, that are associated with the common cold; coronaviruses are generally associated with more severe symptoms than are rhinoviruses. A British study of people older than 60 years of age who had colds was able to isolate a causative virus in only 43% of patients,3 and Finnish researchers were able to isolate viruses from 138 of 200 university students with colds.4 Colds occur all year round but are more common in the winter months.2,5
Definitions of the common cold are rather vague, but colds have the following features:
feeling generally mildly unwell (“indisposed”),
a sensation of chills (which means feeling cold when the core temperature is either normal or even raised), and
sniffles (excessive nasal discharge above the normal physiologic level).
These are the main symptoms that people experience. Perhaps the chills people feel (a kind of oversensitivity to the ambient temperature) are the reason why the illness is called the cold.
Everyone has had the illness and so it is not hard to recognize the symptoms. There are, however, many variations on the theme. Usually the infection starts in the nasal cavity mucosa (the typical common cold), but it might start in the throat, the sinuses, the ears, or the bronchi, in which case the first symptom could be a sore throat, pain in the facial bones, earache, or cough. Soon after, with the advent of the streaming nose that accompanies the generally chilled feeling, we realize the constellation of symptoms is a cold.
Common cold - PMC
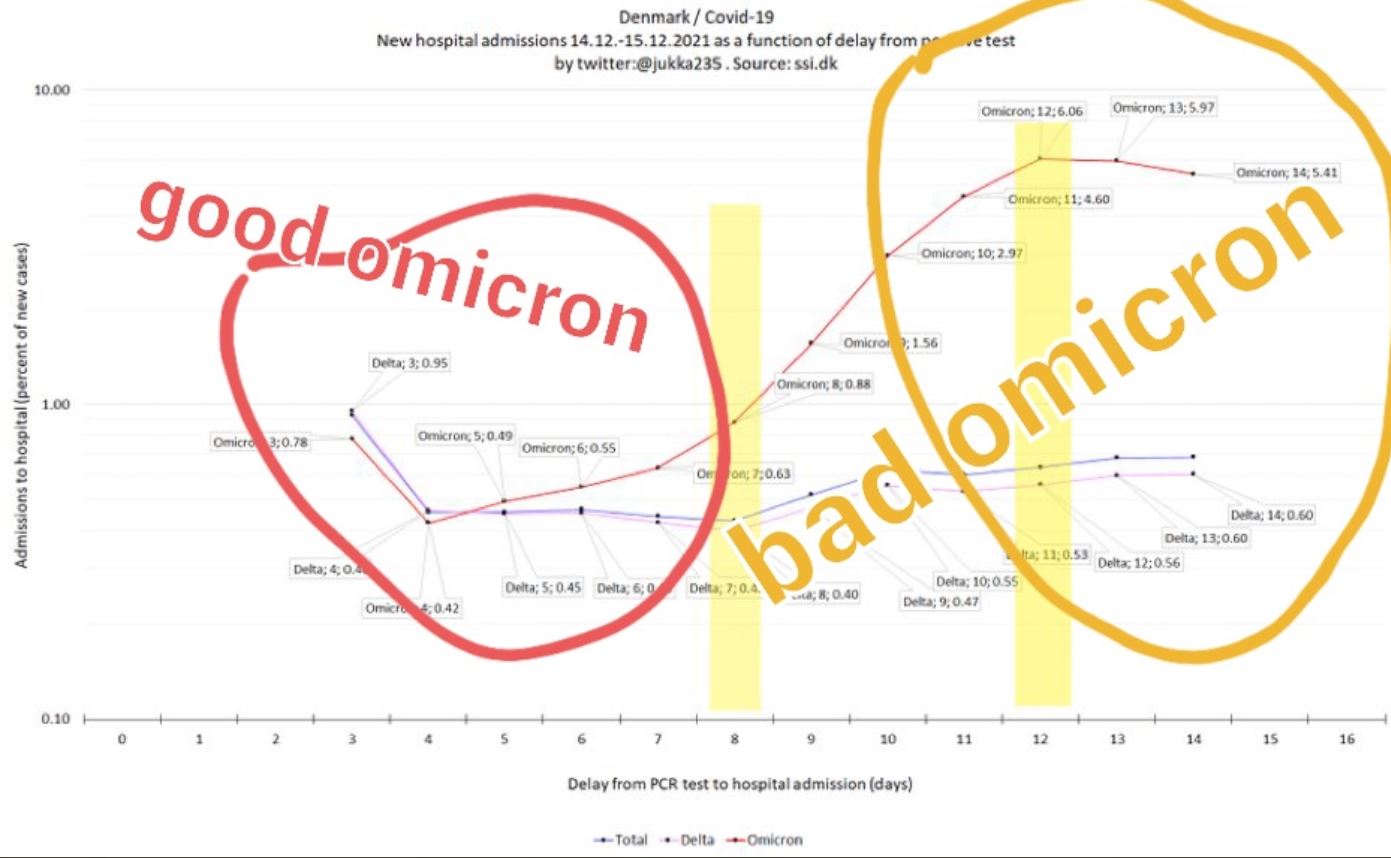
This following article is rather long, so I have only presented the 1st half of it. Knowing that the 2018-2019 influenza Pandemic “disappeared” as a Pandemic in only two years, and devolved into the endemic strains of seasonal flu we have today, shows what is happening to Covid-19. This occurred at a time when there were no vaccines or antibiotics, only the natural immunity incorporated in our natural DNA defenses. In a previous post I had highlighted how Covid-19 now has multiple animal reservoirs that have allowed mutation in about 5% of the spike proteins in Omicron. This jump to animal reservoirs has been occurring for more than a year. Omicron is highly transmissive, but a less virulent strain of the original Covid-19. If not Omicron, then one of the next several mutated strains of this virus will likely be no more dangerous than the common cold. We will need to learn to live with and treat this endemic virus no different than we do other dangerous, but largely survivable illnesses. Omicron will likely prove to be no more lethal than the seasonal flu or the existing common cold in the healthiest among us.
The Omicron Variant: Much Ado About Nothing?
The World Health Organization is warning the Omicron variant can spread more quickly than other variants. That’s likely true, but based on science, that doesn’t mean the variant is more lethal than Delta or others — in fact, it’s probably more mild.
By Paul Elias Alexander, Ph.D.
The WHO has said the Omicron variant can spread more quickly than other variants. Likely true. The virus is behaving just like how viruses behave.
They are mutable and mutate, and via the Muller’s ratchet theory, we expect these to be milder and milder mutations, not more lethal ones given the pathogen seeks to infect the host and not arrive at an evolutionary dead end.
The virus will mutate downward so that it can use the host (us) to propagate itself via our cellular metabolic machinery. The Delta variant has shown us this: It is very infectious and mostly non-lethal — specially for children and healthy people.
So is the WHO panicking the globe needlessly? Is this COVID-19 February 2020 once again?
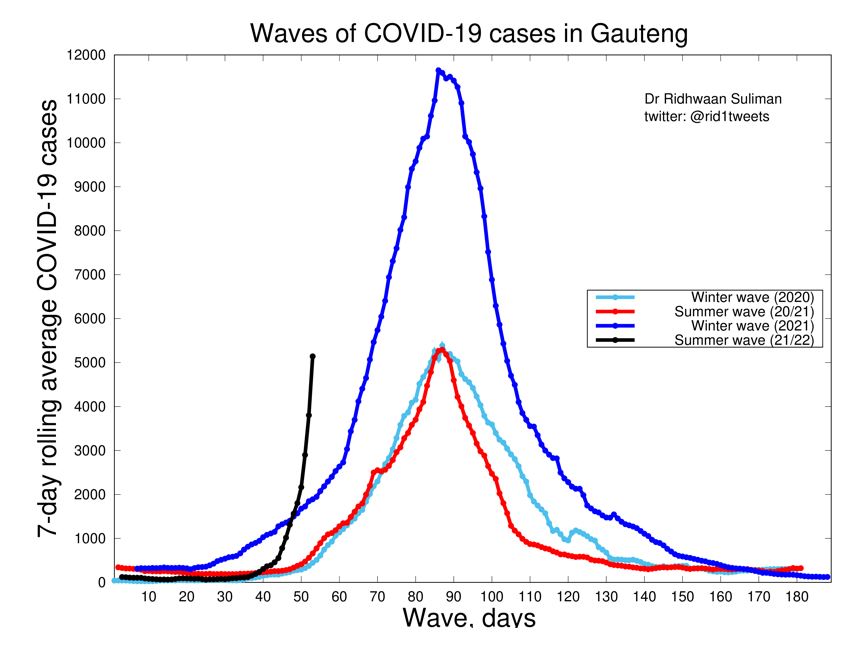
The problem with South Africa, similar to Australia and New Zealand and even island nations like Trinidad, is that South Africa has low natural immunity to SAR-CoV-2.
This is because, as we witnessed over the last year and more, if you lock down your society too long and too hard, you deny the nation and population from inching closer to population-level herd immunity.
And you have no economy or society from which to reemerge. You devastate your society for a pathogen that is largely harmless to the vast majority of people, especially children.
Moreover, governments asked us for two weeks to flatten the curve to help prepare hospitals so that they can tend to surges and other non-COVID illnesses. We as societies gave our governments two weeks, not 21 months.
They failed to tend to the non-COVID illnesses, and we locked down the healthy and well (children and young and middle aged healthy persons) while failing to properly protect the vulnerable and high-risk persons such as the elderly.
We failed and it was like killing fields in our nursing homes.
This failure rests on public health messaging and government. Additionally, what did our governments in the U.S., Canada, UK, Australia etc. do with the tax money for the hospitals and personal protective equipment (PPE), etc.?
Hospitals must be prepared by now. Governments have failed! Not the people. The task forces have failed, not the people.
These nations thought that they could stay locked down and wait for a vaccine. This is a reasonable view, though I was against lockdowns as they would and did cause crushing harms on especially poor persons and children.
The problem is there was an opportunity cost because the vaccine we were waiting on was suboptimally developed without the proper safety testing or assessment of effectiveness.
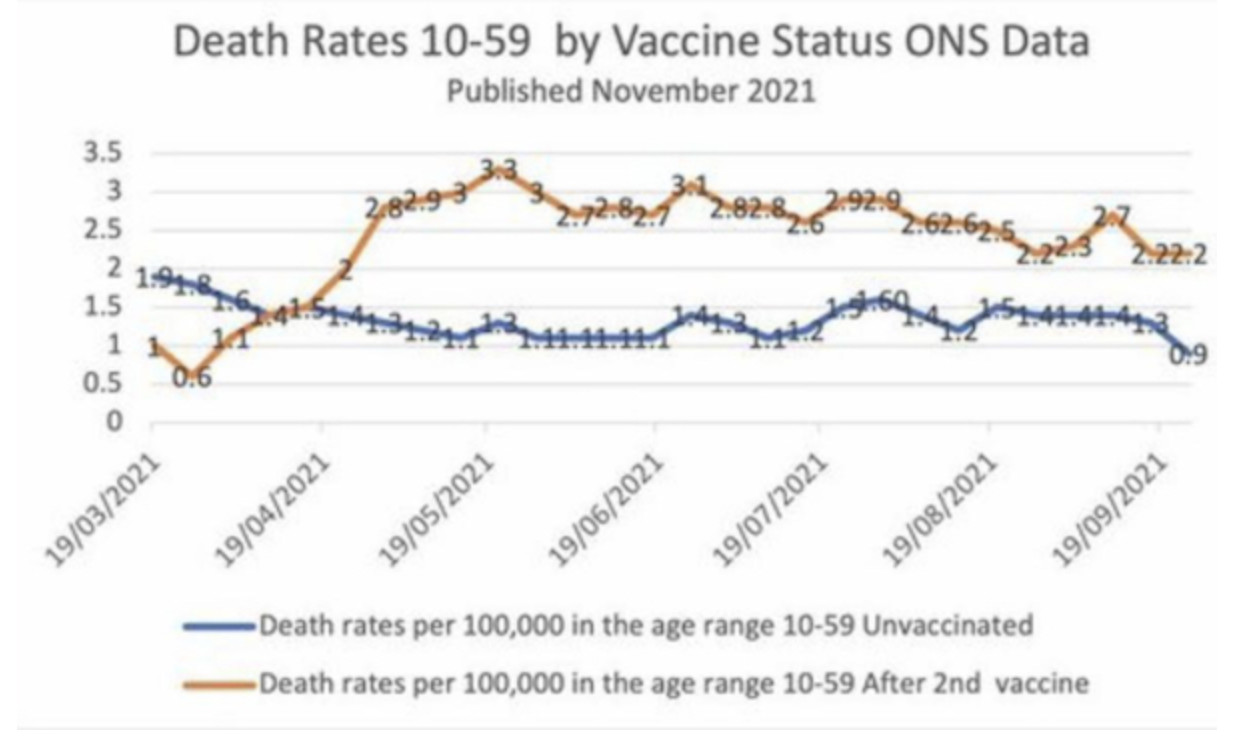
We have data that the Pfizer vaccine loses 40% of antibodies per month, meaning in 3 months post-shot, you have low effective vaccinal immunity.
We see it clearly playing out now whereby you got to tamp down spread with the draconian lockdowns, but you did it at the cost of natural immunity.
That is the opportunity cost. So we spent on getting the vaccine and it cost us natural immunity and thus herd immunity. For example, the vaccine has failed to stop infection and spread against Delta.
We have research findings that reveal the vaccines have very suboptimal efficacy:
- Singanayagam et al. (fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts).
- Chau et al. (viral loads of breakthrough Delta variant infection cases in vaccinated nurses were 251 times higher than those of cases infected with prior strains early 2020).
- Riemersma et al. (no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections and if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others).
This situation of the vaccinated being infectious and transmitting the virus has also emerged in seminal nosocomial outbreak papers by:
These studies have also revealed that the PPE and masking were essentially ineffective within the healthcare setting. All of the healthcare workers were double-vaccinated, yet there was extensive spread to themselves and their patients.
In addition, the following studies collectively reveal the poor efficacy and even negative efficacy of the COVID vaccines:
(article continues at the link below)
The Omicron Variant: Much Ado About Nothing? • Children's Health Defense
![south-africa-hospital-1200x800-1200x800 WHO: No Deaths Reported as a Result of Omicron Variant, CDC Reports No Deaths Only One Hospitalization Featured Top Stories World [your]NEWS](https://theminingplay.com/uploads/db1184/original/2X/a/ae2a4f1e87ff5264a4abe3c1c0518a12bf8bfb31.jpeg "south-africa-hospital-1200x800-1200x800 WHO: No Deaths Reported as a Result of Omicron Variant, CDC Reports No Deaths Only One Hospitalization Featured Top Stories World [your]NEWS")